Glossitis
| Glossitis | |
|---|---|
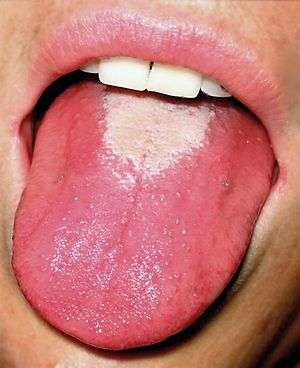 | |
| Glossitis in a person with scarlet fever ("red strawberry tongue"). | |
| Classification and external resources | |
| Specialty | gastroenterology |
| ICD-10 | K14.0 |
| ICD-9-CM | 529.0 |
| DiseasesDB | 5252 |
| MedlinePlus | 001053 |
Glossitis can mean soreness of the tongue, or more usually inflammation with depapillation of the dorsal surface of the tongue (loss of the lingual papillae), leaving a smooth and erythematous (reddened) surface,[1][2] (sometimes specifically termed atrophic glossitis). In a wider sense, glossitis can mean inflammation of the tongue generally.[3] Glossitis is often caused by nutritional deficiencies and may be painless or cause discomfort. Glossitis usually responds well to treatment if the cause is identified and corrected. Tongue soreness caused by glossitis is differentiated from burning mouth syndrome, where there is no identifiable change in the appearance of the tongue, and there are no identifiable causes.[4]
Classification

Glossitis could be classified as a group of tongue diseases or gastrointestinal diseases.[3] It may be primary, where there is no underlying cause, or secondary where it is a sign or symptom of another condition.[2] It can be acute or chronic.[3] Generally speaking, there are several clinical patterns of glossitis, some more common than others.
Atrophic glossitis
Atrophic glossitis, also known as bald tongue,[2] smooth tongue, Hunter glossitis, Moeller glossitis, or Möller-Hunter glossitis,[5] is a condition characterized by a smooth glossy tongue that is often tender/painful,[6] caused by complete atrophy of the lingual papillae (depapillation).[2] The dorsal tongue surface may be affected totally, or in patches, and may be associated with a burning sensation, pain and/or erythema.[7] Atrophic glossitis is a non-specific finding,[7] and has a great many causes, usually related to iron-deficiency anemia, pernicious anemia, B vitamin complex deficiencies,[8] unrecognized and untreated celiac disease (which often presents without gastrointestinal symptoms),[9][10][11] or other factors such as xerostomia (dry mouth). Although the terms Möller and Hunter glossitis were originally used to refer to specifically the glossitis that occurs in vitamin B12 deficiency secondary to pernicious anemia, they are now used as synonyms for atrophic glossitis generally.[5] In this article, the term glossitis, unless otherwise specified, refers to atrophic glossitis.
Candidiasis may be a concurrent finding or an alternative cause of erythema, burning, and atrophy.
Median rhomboid glossitis
This condition is characterized by a persistent erythematous, rhomboidal depapillated lesion in the central area of the dorsum of the tongue, just in front of the circumvallate papillae.[1][6] Median rhomboid glossitis is a type of oral candidiasis, and rarely causes any symptoms. It is treated with antifungal medication. Predisposing factors include use of corticosteroid sprays or inhalers or immunosuppression.
Benign migratory glossitis
Geographic tongue, also termed benign migratory glossitis, is a common condition which usually affects the dorsal surface of the tongue. It is characterized by patches of depapillation and erythema bordered by a whitish peripheral zone. These patches give the tongue the appearance of a map, hence the name. Unlike glossitis due to nutritional deficiencies and anemia, the lesions of geographic tongue move around the tongue over time.[12] This is because in geographic tongue, new areas of the tongue become involved with the condition whilst previously affected areas heal, giving the appearance of a moving lesion.[2] The cause is unknown,[13] and there is no curative treatment. Rarely are there any symptoms associated with the lesions, but occasionally a burning sensation may be present, which is exacerbated by eating hot, spicy or acidic foodstuffs. Some consider geographic tongue to be an early stage of fissured tongue, since the two conditions often occur in combination.[14]
Geometric glossitis
Geometric glossitis, also termed herpetic geometric glossitis,[3] is a term used by some to refer to a chronic lesion associated with herpes simplex virus (HSV) type I infection,[15] in which there is a deep fissure in the midline of the tongue, which gives off multiple branches.[16] The lesion is usually very painful, and there may be erosions present in the depths of the fissures. Similar fissured lesions which are not associated with HSV, as may occur in fissured tongue, do not tend to be painful.[15] The name comes from the geometric pattern of the fissures which are longitudinal, crossed or branched.[17] It is described as occurring in immunocompromized persons, e.g. who have leukemia. However, the association between herpes simplex and geometric glossitis is disputed by some due to a lack of gold standard techniques for diagnosis of intraoral herpetic lesions, and the high prevalence of asymptomatic viral shedding in immunocompromized individuals.[16] Treatment is with systemic aciclovir.[15]
Strawberry tongue
Strawberry tongue (also called raspberry tongue),[18] refers to glossitis which manifests with hyperplastic (enlarged) fungiform papillae, giving the appearance of a strawberry. White strawberry tongue is where there is a white coating on the tongue through which the hyperplastic fungiform papillae protrude. Red strawberry tongue is where the white coating is lost and a dark red, erythematous surface is revealed, interspaced with the hyperplastic fungiform papillae. White strawberry tongue is seen in early scarlet fever (a systemic infection of group A β- hemolytic streptococci),[19] and red strawberry tongue occurs later, after 4–5 days.[16] Strawberry tongue is also seen in Kawasaki disease (a vasculitic disorder primarily occurring in children under 5),[20][21] and toxic shock syndrome.[22] It may mimic other types of glossitis or Vitamin B12 deficiency.[23]
Symptoms
Depending upon what exact meaning of the word glossitis is implied, signs and symptoms might include:
- Smooth, shiny appearance of the tongue, caused by loss of lingual papillae.
- Tongue color changes, usually to a darker red color than the normal white-pink color of a healthy tongue.
- Tongue swelling.
- Difficulty with chewing, swallowing, or speaking (either because of tongue soreness of tongue swelling).
- Burning sensation.[1] Some use the term secondary burning mouth syndrome in cases where a detectable cause, such as glossitis, for an oral burning sensation.[4]
Depending upon the underlying cause, there may be additional signs and symptoms such as pallor, oral ulceration and angular cheilitis.[1]
Causes
Anemias
Iron-deficiency anemia is mainly caused by blood loss, such as may occur during menses or gastrointestinal hemorrhage. This often results in a depapilled, atrophic glossitis, giving the tongue a bald and shiny appearance, along with pallor (paleness) of the lips and other mucous membranes a tendency towards recurrent oral ulceration,[24] and cheilosis (swelling of the lips).[25] The appearance of the tongue in iron deficiency anemia has been described as diffuse or patchy atrophy with tenderness or burning.[16] One cause of iron deficiency anemia is sideropenic dysphagia (Plummer–Vinson or Paterson–Brown–Kelly syndrome) which is also characterized by esophageal webbing and dysphagia.[24]
Pernicious anemia is usually caused by autoimune destruction of gastric parietal cells. Parietal cells secrete intrinsic factor which is required for the absorption of vitamin B12. Vitamin B12 deficiency results in megaloblastic anemia and may present as glossitis. The appearance of the tongue in vitamin B12 deficiency is described as "beefy" or "fiery red and sore".[24] There may be linear or patchy red lesions.[1]
Vitamin B deficiencies
Vitamin B1 deficiency (thiamin deficiency) can cause glossitis.[25] Vitamin B2 deficiency (ariboflavinosis) can cause glossitis, along with angular cheilitis, cheilosis, peripheral neuropathy and other signs and symptoms.[25] The glossitis in vitamin B2 deficiency is described as magenta.[26] Vitamin B3 deficiency (pellagra) can cause glossitis.[25] Vitamin B6 deficiency (pyridoxine deficiency) can cause glossitis, along with angular cheilitis, cheilosis, peripheral neuropathy and seborrheic dermatitis.[25] Folate deficiency (vitamin B9 deficiency) can cause glossitis, along with macrocytic anemia, thrombocytopenia, leukopenia, diarrhea, fatigue and possibly neurological signs.[25] Apart from pernicious anemia discussed above, any other cause of vitamin B12 deficiency can cause glossitis, which tends to be painful, smooth and shiny.[25]
Infections
Bacterial, viral or fungal infections can cause glossitis. Candida species are involved in median rhomboid glossitis. Candida species also may be involved in creating a more generalized glossitis with erythema, burning, and atrophy,[7]
e.g. erythematous candidiasis (e.g. as may occur in HIV/AIDS) may involve the tongue giving glossitis with depapillation.[1]
Syphilis is now relatively rare, but the tertiary stage can cause diffuse glossitis and atrophy of lingual papillae, termed "syphlitic glossitis",[1] "luetic glossitis" or "atrophic glossitis of tertiary syphilis".[16] It is caused by Treponema pallidum and is a sexually transmitted infection.
Other causes
Many conditions can cause glossitis via malnutrition or malabsorption,[25] which creates the nutritional deficiencies described above, although other mechanisms may be involved in some of those conditions listed.
- Alcoholism[25]
- Sprue (celiac disease,[27] or tropical sprue), secondary to nutritional deficiencies[25]
- Crohn’s disease[25]
- Whipple disease[25]
- Glucagonoma syndrome[25]
- Cowden disease[25]
- Acquired immunodeficiency syndrome (AIDS)[25]
- Carcinoid syndrome[25]
- Kwashiorkor amyloidosis[25]
- Veganism and other specialized diets,[1]
- Poor hydration and low saliva in the mouth, which allows bacteria to grow more readily
- Mechanical irritation or injury from burns, rough edges of teeth or dental appliances, or other trauma
- Tongue piercing[28] Glossitis can be caused by the constant irritation by the ornament and by colonization of Candida albicans in site and on the ornament[29]
- Exposure to irritants such as tobacco, alcohol, hot foods, or spices
- Allergic reaction to toothpaste, mouthwash, breath fresheners, dyes in confectionery, plastic in dentures or retainers, or certain blood-pressure medications (ACE inhibitors)
- Administration of ganglion blockers (e.g., Tubocurarine, Mecamylamine).
- Oral lichen planus, erythema multiforme, aphthous ulcer, pemphigus vulgaris
- Heredity
- Albuterol (bronchodilator medicine)
- Schizophrenia
- A painful tongue may be an indication of several underlying serious medical conditions and nearly always merits assessment by a physician or dental surgeon
Treatment
The goal of treatment is to reduce inflammation. Treatment usually does not require hospitalization unless tongue swelling is severe. Good oral hygiene is necessary, including thorough tooth brushing at least twice a day, and flossing at least daily. Corticosteroids such as prednisone may be given to reduce the inflammation of glossitis. For mild cases, topical applications (such as a prednisone mouth rinse that is not swallowed) may be recommended to avoid the side effects of swallowed or injected corticosteroids. Antibiotics, antifungal medications, or other antimicrobials may be prescribed if the cause of glossitis is an infection. Anemia and nutritional deficiencies (such as a deficiency in niacin, riboflavin, iron, or Vitamin E) must be treated, often by dietary changes or other supplements. Avoid irritants (such as hot or spicy foods, alcohol, and tobacco) to minimize the discomfort. In some cases, tongue swelling may threaten the airway, a medical emergency that needs immediate attention.
Prevention
Good oral hygiene (thorough tooth brushing and flossing and regular professional cleaning and examination) may be helpful to prevent these disorders. Drinking plenty of water and the production of enough saliva, aid in the reduction of bacterial growth. Minimizing irritants or injury in the mouth when possible can aid in the prevention of glossitis. Avoiding excessive use of any food or substance that irritates the mouth or tongue may also help.
Epidemiology
One review reported overall prevalence ranges of 0.1–14.3% for geographic tongue, 1.3–9.0% for "atrophy tongue" (atrophic glossitis), and 0.0–3.35% for median rhomboid glossitis.[30]
References
- 1 2 3 4 5 6 7 8 Scully, Crispian (2008). Oral and maxillofacial medicine : the basis of diagnosis and treatment (2nd ed.). Edinburgh: Churchill Livingstone. p. 356. ISBN 9780443068188.
- 1 2 3 4 5 Rogers, K (editor) (2010). The digestive system (1st ed.). New York, NY: Britannica Educational Pub., in association with Rosen Educational Services. p. 146. ISBN 978-1615301317.
- 1 2 3 4 Frank J. Domino (editor-in-chief); Robert A. Baldor (, associate editors); et al. (2012-03-07). The 5-minute clinical consult 2012 (20th ed.). Philadelphia, Pa.: Wolters Kluwer Health/Lippincott Williams & Wilkins. pp. 532, 533. ISBN 978-1451103038.
- 1 2 Zakrzewska, JM; Forssell, H; Glenny, AM (Jan 25, 2005). "Interventions for the treatment of burning mouth syndrome.". The Cochrane Database of Systematic Reviews (1): CD002779. doi:10.1002/14651858.CD002779.pub2. PMID 15674897.
- 1 2 O. Braun-Falco (2000). Dermatology (2nd ed.). Berlin [u.a.]: Springer. p. 1173. ISBN 3540594523.
- 1 2 James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: Clinical Dermatology (14th ed.). Saunders Elsevier. p. 803. ISBN 0721629210.
- 1 2 3 Chi, AC; Neville, BW; Krayer, JW; Gonsalves, WC (Dec 1, 2010). "Oral manifestations of systemic disease.". American Family Physician. 82 (11): 1381–8. PMID 21121523.
- ↑ Chi AC, Neville BW, Krayer JW, Gonsalves WC (Dec 1, 2010). "Oral manifestations of systemic disease". Am Fam Physician (Review). 82 (11): 1381–8. PMID 21121523.
- ↑ Rashid M, Zarkadas M, Anca A, Limeback H (2011). "Oral manifestations of celiac disease: a clinical guide for dentists". J Can Dent Assoc (Review). 77: b39. PMID 21507289.
- ↑ "Dental Enamel Defects and Celiac Disease" (PDF). National Institute of Health (NIH). Retrieved Mar 7, 2016.
Tooth defects that result from celiac disease may resemble those caused by too much fluoride or a maternal or early childhood illness. Dentists mostly say it’s from fluoride, that the mother took tetracycline, or that there was an illness early on
- ↑ Giuca MR, Cei G, Gigli F, Gandini P (2010). "Oral signs in the diagnosis of celiac disease: review of the literature". Minerva Stomatol (Review). 59 (1-2): 33–43. PMID 20212408.
There are enough evidence making the correlation between CD and oral defects scientifically sustainable. This recognition should lead dentists to play more significant roles in screening for CD, as otherwise, if not properly diagnosed and not treated with a gluten-free diet, may eventually cause some malignancies.
- ↑ Adeyemo, TA; Adeyemo, WL; Adediran, A; Akinbami, AJ; Akanmu, AS (May–Jun 2011). "Orofacial manifestations of hematological disorders: anemia and hemostatic disorders.". Indian Journal of Dental Research. 22 (3): 454–61. doi:10.4103/0970-9290.87070. PMID 22048588.
- ↑ Reamy, BV; Derby, R; Bunt, CW (Mar 1, 2010). "Common tongue conditions in primary care.". American Family Physician. 81 (5): 627–34. PMID 20187599.
- ↑ Greenberg, MS; Glick, M; Ship, JA (2008). Burket's oral medicine (11th ed.). Hamilton, Ont.: BC Decker. ISBN 1550093452.
- 1 2 3 Cohen, PR; Kazi, S; Grossman, ME (December 1995). "Herpetic geometric glossitis: a distinctive pattern of lingual herpes simplex virus infection.". Southern Medical Journal. 88 (12): 1231–5. doi:10.1097/00007611-199512000-00009. PMID 7502116.
- 1 2 3 4 5 Neville BW, Damm DD, Allen CA, Bouquot JE (2002). Oral & maxillofacial pathology (2nd ed.). Philadelphia: W.B. Saunders. pp. 169, 170. ISBN 0721690033.
- ↑ Grossman, ME; Stevens, AW; Cohen, PR (Dec 16, 1993). "Brief report: herpetic geometric glossitis.". The New England Journal of Medicine. 329 (25): 1859–60. doi:10.1056/NEJM199312163292506. PMID 8247038.
- ↑ [editor, Scott Stocking, associate editor, Jyothimai Gubili] (2004). Mosby's dental dictionary. St. Louis, Mo.: Mosby. ISBN 978-0323025102.
- ↑ Yang SG, Dong HJ, Li FR, et al. (November 2007). "Report and analysis of a scarlet fever outbreak among adults through food-borne transmission in China". J. Infect. 55 (5): 419–24. doi:10.1016/j.jinf.2007.07.011. PMID 17719644.
- ↑ Singh, S; Kansra, S (Jan–Feb 2005). "Kawasaki disease.". The National Medical Journal of India. 18 (1): 20–4. PMID 15835487.
- ↑ Park AH, Batchra N, Rowley A, Hotaling A; Batchra; Rowley; Hotaling (May 1997). "Patterns of Kawasaki syndrome presentation". Int. J. Pediatr. Otorhinolaryngol. 40 (1): 41–50. doi:10.1016/S0165-5876(97)01494-8. PMID 9184977.
- ↑ Baehler EA, Dillon WP, Cumbo TJ, Lee RV; Dillon; Cumbo; Lee (August 1982). "Prolonged use of a diaphragm and toxic shock syndrome". Fertil. Steril. 38 (2): 248–50. PMID 7106318.
- ↑ Gary Williams; Murray Katcher. "Skin Lesions: Strawberry Tongue". Primary Care Dermatology Module (University of Wisconsin Madison). Retrieved 2007-08-14.
- 1 2 3 Treister NS, Bruch JM (2010). Clinical oral medicine and pathology. New York: Humana Press. p. 149. ISBN 978-1-60327-519-4.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Tadataka Yamada, David H. Alpers, et al., eds. (2009). Textbook of gastroenterology (5th ed.). Chichester, West Sussex: Blackwell Pub. pp. 1717–1744. ISBN 978-1-4051-6911-0.
- ↑ Park, KK; Brodell RT; Helms SE. (July 2011). "Angular cheilitis, part 2: nutritional, systemic, and drug-related causes and treatment." (PDF). Cutis. 88 (1): 27–32. PMID 21877503.
- ↑ Pastore, L; Carroccio, A; Compilato, D; Panzarella, V; Serpico, R; Lo Muzio, L (March 2008). "Oral manifestations of celiac disease.". Journal of Clinical Gastroenterology. 42 (3): 224–32. doi:10.1097/MCG.0b013e318074dd98. PMID 18223505.
- ↑ Levin Liran, Zadik Yehuda; Zadik (October 2007). "Oral Piercing: Complications and Side Effects". Am J Dent. 20 (5): 340–344. PMID 17993034.
- ↑ Zadik Yehuda, Burnstein Saar, Derazne Estella, Sandler Vadim, Ianculovici Clariel, Halperin Tamar; Burnstein; Derazne; Sandler; Ianculovici; Halperin (March 2010). "Colonization of Candida: prevalence among tongue-pierced and non-pierced immunocompetent adults". Oral Dis. 16 (2): 172–5. doi:10.1111/j.1601-0825.2009.01618.x. PMID 19732353.
- ↑ Dombi, C; Czeglédy, A (November 1992). "[Incidence of tongue diseases based on epidemiologic studies (review of the literature)].". Fogorvosi szemle. 85 (11): 335–41. PMID 1291323.