Management of scoliosis
The management of scoliosis is complex and is determined by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression. The conventional options for children and adolescents are:[1]
- Observation
- Bracing
- Specialized physical therapy
- Surgery
For adults, treatment usually focuses on relieving any pain:[2][3]
- Painkilling medication
- Bracing
- Exercise
- Surgery[4]
Treatment for idiopathic scoliosis also depends upon the severity of the curvature, the spine’s potential for further growth, and the risk that the curvature will progress. Mild scoliosis (less than 30 degrees deviation) may simply be monitored and treated with exercise. Moderately severe scoliosis (30–45 degrees) in a child who is still growing may require bracing. Severe curvatures that rapidly progress may be treated surgically with spinal rod placement. Bracing may prevent a progressive curvature, but evidence for this is not very strong. In all cases, early intervention offers the best results. A growing body of scientific research testifies to the efficacy of specialized treatment programs of physical therapy, which may include bracing.[5]
Physical therapy
Physical therapists and occupational therapists help those who have experienced an injury or illness regain or maintain the ability to participate in everyday activities. For those with scoliosis, a physical therapist and/or occupational therapist can provide assistance through assessment, intervention, and ongoing evaluation of the condition. This helps them manage physical symptoms and/or use compensatory techniques so that they can participate in daily activities like self-care, productivity, and leisure.
One intervention involves bracing. During the past several decades, a large variety of bracing devices have been developed for the treatment of scoliosis.[6] Studies demonstrate that preventing force sideways across a joint by bracing prevents further curvature of the spine in idiopathic scoliosis,[7] while other studies have also shown that braces can be used by individuals with scoliosis during physical activities.[8]
Other interventions include postural strategies, such as posture training in sitting, standing, and sleeping positions, and in using positioning supports such as pillows, wedges, rolls, and corsets.[9]
Adaptive and compensatory strategies are also employed to help facilitate individuals to returning daily activities.
Exercise
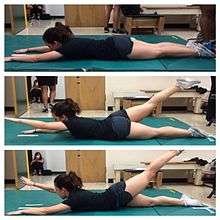
Strengthening spinal muscles is a crucial preventive measure. This is because the muscles in the back are essential when it comes to supporting the spinal column and maintaining the spine's proper shape. Exercises that will help improve the strength of the muscles in the back include rows and leg and arm extensions.[10] Elastic resistance exercise may also be able to sustain the progression of spinal curvature.[11] This type of exercise is able to sustain progression by equalizing the strength of the torso muscles found on each side of the body.
Self-care
Disability caused by scoliosis, as well as physical limitations during recovery from treatment-related surgery, often affects an individual’s ability to perform self-care activities.[12] One of the first treatments of scoliosis is the attempt to prevent further curvature of the spine. Depending on the size of the curvature, this is typically done in one of three ways: bracing, surgery, or postural positioning through customized cushioning.[12][13][14] Stopping the progression of the scoliosis can prevent the loss of function in many activities of daily living by maintaining range of motion, preventing deformity of the rib cage, and reducing pain during activities such as bending or lifting.
Occupational therapists are often involved in the process of selection and fabrication of customized cushions. These individualized postural supports are used to maintain the current spinal curvature, or they can be adjusted to assist in the correction of the curvature. This type of treatment can help to maintain mobility for a wheelchair user by preventing the deformity of the rib cage and maintaining an active range of motion in the arms.[12]
For other self-care activities (such as dressing, bathing, grooming, personal hygiene, and feeding), several strategies can be used as a part of occupational therapy treatment. Environmental adaptations for bathing could include a bath bench, grab bars installed in the shower area, or a handheld shower nozzle.[15] For activities such as dressing and grooming, various assistive devices and strategies can be used to promote independence. An occupational therapist may recommend a long-handled reacher that can be used to assist self-dressing by allowing a person to avoid painful movements such as bending over; a long-handled shoehorn can be used for putting on and removing shoes. Problems with activities such as cutting meat and eating can be addressed by using specialized cutlery, kitchen utensils, or dishes.
Productivity
Productive activities include paid or unpaid work, household chores, school, and play.[16] Recent studies in healthcare have led to the development of a variety of treatments to assist in the management of scoliosis thereby maximizing productivity for people of all ages. Assistive technology has undergone dramatic changes over the past 20 years; the availability and quality of the technology has improved greatly.[17] As a result of using assistive technology, functional changes may range from improvements in abilities, performance in daily activities, participation levels, and quality of life.[16]
A common assistive technology intervention is specialized seating and postural control. For children with poor postural control, a comfortable seating system that provides them with the support needed to maintain a sitting position can be essential for raising their overall level of well-being.[18] A child's well-being in a productive sense involves the ability to participate in classroom and play activities.[16] Specialized wheelchair seating has been identified as the most common prescription in the management of scoliosis in teenagers with muscular dystrophy.[19]
With comfortable wheelchair seating, teenagers are able to participate in classroom activities for longer periods with less fatigue. By tilting the seating position 20° forward (toward the thighs), seating pressure is significantly redistributed, so sitting is more comfortable. If an office worker with scoliosis can sit for longer periods, increased work output is likely to occur and could improve quality of life. Tall, forward-sloping seats or front parts of seats, and when possible with tall desk with the opposite slope, can, in general, reduce pains and the need of bending significantly while working or studying, and that is particularly important with braced, fragile, or tender backs. An open hip angle can benefit the used lung volume and respiration.[20][21]
For those not using a wheelchair, bracing may be used to treat scoliosis. Lifestyle changes are made to compensate for the proper use of spine braces.
Leisure
Physical symptoms such as chest pains, back pains, shortness of breath, and limited spinal movement can hamper or preclude participation in leisure activities of a physical nature. The occupational therapist's role is to facilitate participation by helping the patient manage these symptoms.
Bracing is a common strategy recommended by an occupational therapist, in particular, for individuals engaging in sports and exercise.[8] An OT is responsible for educating an individual on the advantages and disadvantages of different braces, proper ways to wear the brace, and the day-to-day care of the brace.
To help a person manage heart and lung symptoms, such as shortness of breath or chest pains, an occupational therapist can teach the individual energy conservation techniques.[15] This includes scheduling routine breaks during the activity, as suitable for the individual. For example, an occupational therapist can recommend that a swimmer take breaks between laps to conserve energy. Adapting or modifying the exercise or sport is another way a person with scoliosis can do it.[15] Adapting the activity may change the difficulty of the sport or exercise. For example, it might mean taking breaks throughout an exercise. If a person with scoliosis is unable to participate in a sport or exercise, an OT can help the individual explore other physical activities that are suitable to his/her interests and capabilities. An occupational therapist and the person with scoliosis can explore enjoyable and meaningful participation in the sport/exercise in another capacity, such as coaching or refereeing.
Bracing
Bracing is normally done when the patient has bone growth remaining and is, in general, implemented to hold the curve and prevent it from progressing to the point where surgery is recommended. In some cases with juveniles, bracing has reduced curves significantly, going from a 40 degrees (of the curve, mentioned in length above.) out of the brace to 18 degrees in it. Braces are sometimes prescribed for adults to relieve pain related to scoliosis. Bracing involves fitting the patient with a device that covers the torso; in some cases, it extends to the neck. The most commonly used brace is a TLSO, such as a Boston brace, a corset-like appliance that fits from armpits to hips and is custom-made from fiberglass or plastic. It is sometimes worn 22–23 hours a day, depending on the doctor's prescription, and applies pressure on the curves in the spine. The effectiveness of the brace depends not only on brace design and orthotist skill but on patient compliance and amount of wear per day. The typical use of braces is for idiopathic curves that are not grave enough to warrant surgery, but they may also be used to prevent the progression of more severe curves in young children, to buy the child time to grow before performing surgery, which would prevent further growth in the part of the spine affected.
Indications for Scoliosis Bracing: Scoliosis professionals determine the proper bracing method for a patient after a complete clinical evaluation. The patient’s growth potential, age, maturity, and scoliosis (Cobb angle, rotation, and sagittal profile) are also considered. Immature patients who present with Cobb angles less than 20 degrees should be closely monitored. Immature patients who present with Cobb angles of 20 degrees to 29 degrees should be braced according to the risk of progression by considering age, Cobb angle increase over a six-month period, Risser sign, and clinical presentation. Immature patients who present with Cobb angles greater than 30 degrees should be braced. However, these are guidelines and not every patient will fit into this table. For example, an immature patient with a 17-degree Cobb angle and significant thoracic rotation or flatback could be considered for nighttime bracing. On the opposite end of the growth spectrum, a 29-degree Cobb angle and a Risser sign three or four might not need to be braced because there is reduced potential for progression.[22]
Surgery is indicated by the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) at 45 degrees to 50 degrees[23] and by the Scoliosis Research Society (SRS) at a Cobb angle of 45 degrees.[24] SOSORT uses the 45-degree to 50-degree threshold as a result of the well-documented, plus or minus five degrees measurement error that can occur while measuring Cobb angles.
Scoliosis braces are usually comfortable for the patient, especially when it is well designed and fit; also after the 7- to 10-day break-in period. A well fit and functioning scoliosis brace provides comfort when it is supporting the deformity and redirecting the body into a more corrected and normal physiological position.[25]
The Scoliosis Research Society's recommendations for bracing include curves progressing to larger than 25°, curves presenting between 30 and 45°, Risser sign 0, 1, or 2 (an X-ray measurement of a pelvic growth area), and less than six months from the onset of menses in girls.[26]

Progressive scolioses exceeding 25° Cobb angle in the pubertal growth spurt should be treated with a pattern-specific brace like the Chêneau brace and its derivatives, with an average brace-wearing time of 16 hours/day (23 hours/day assures the best possible result).
The latest standard of brace construction is with CAD/CAM technology. With the help of this technology, it has been possible to standardize the pattern-specific brace treatment. Severe mistakes in brace construction are largely ruled out with the help of these systems. This technology also eliminates the need to make a plaster cast for brace construction. The measurements can be taken in any place and are simple (and not comparable to plastering). In Germany, available CAD/CAM braces are known such as the Regnier-Chêneau brace, the Rigo-System-Chêneau-brace (RSC brace), and the Gensingen brace.[27] Many patients prefer the "Chêneau light" brace: It has the best in-brace corrections reported in international literature and is easier to wear than other braces in use today.[28][29] However, this brace is not available for all curve patterns.
Prior to 2013 the efficacy of bracing has not been definitively demonstrated in randomised clinical studies, with more limited studies giving inconsistent conclusions.[30] In 2013 the Bracing in Adolescent Idiopathic Scoliosis Trial (BrAIST) published results establishing benefits of bracing in adolescents with idiopathic scoliosis. In the randomized cohort, 72% in the group instructed to wear a brace for 18 hours per day against 48% in the observation group sustained curve progression to under 50 degrees, the proxy used for not requiring surgery. Additionally results suggested that the more a patient wore the brace, the better the result.[31][32]
Casting
In progressive infantile and sometimes juvenile scoliosis, a plaster jacket applied early may be used instead of a brace. It has been proven possible[33] to permanently correct cases of infantile idiopathic scoliosis by applying a series of plaster casts (EDF: elongation, derotation, flexion) on a specialized frame under corrective traction, which helps to "mould" the infant's soft bones and work with their growth spurts. This method was pioneered by UK scoliosis specialist Min Mehta.[34] EDF casting is now the only clinically known nonsurgical method of complete correction in progressive infantile scoliosis. Complete correction may be obtained for curves less than 50° if the treatment begins before the second year of life.[35][36]
Surgery


Surgery is usually recommended by orthopedists for curves with a high likelihood of progression (i.e., greater than 45 to 50° of magnitude), curves that would be cosmetically unacceptable as an adult, curves in patients with spina bifida and cerebral palsy that interfere with sitting and care, and curves that affect physiological functions such as breathing.
Surgery for scoliosis is performed by a surgeon specializing in spine surgery. For various reasons, it is usually impossible to completely straighten a scoliotic spine, but in most cases, significant corrections are achieved.
The two main types of surgery are:
- Anterior fusion: This surgical approach is through an incision at the side of the chest wall.
- Posterior fusion: This surgical approach is through an incision on the back and involves the use of metal instrumentation to correct the curve.
One or both of these surgical procedures may be needed. The surgery may be done in one or two stages and, on average, takes four to eight hours.
Spinal fusion with instrumentation
Spinal fusion is the most widely performed surgery for scoliosis. In this procedure, bone [either harvested from elsewhere in the body (autograft) or from a donor (allograft)] is grafted to the vertebrae so when they heal, they form one solid bone mass and the vertebral column becomes rigid. This prevents worsening of the curve, at the expense of some spinal movement. This can be performed from the anterior (front) aspect of the spine by entering the thoracic or abdominal cavities, or more commonly, performed from the back (posterior). A combination may be used in more severe cases, though the modern pedicle screw system has largely negated the need for this.[30]
In recent years all-screw systems have become the gold-standard technique for adolescent idiopathic scoliosis. Pedicle screws achieve better fixation of the vertebral column and have better biomechanical properties than previous techniques, so enabling greater correction of the curve in all planes.[30]
Pedicle screw-only posterior spinal fusion may improve major curve correction at two years among patients with adolescent idiopathic scoliosis (AIS)[30] as compared to hybrid instrumentation (proximal hooks with distal pedicle screws) (65% versus 46%) according to a retrospective, matched-cohort study.[37] The prospective cohorts were matched to the retrospective cohorts according to patient age, fusion levels, Lenke curve type, and operative method. The two groups were not significantly different in regard to age, Lenke AIS curve type, or Riser grade. The numbers of fused vertebrae were significantly different (11.7±1.6 for pedicle screw versus 13.0±1.2 for hybrid group). This study's results may be biased due to the pedicle screw group's being analyzed prospectively versus retrospective analysis of the hybrid instrumentation group.
In general, modern spinal fusions have good outcomes with high degrees of correction and low rates of failure and infection. However a systematic review of PubMed papers in 2008 concluded "Scoliosis surgery has a varying but high rate of complications", although the non-standardised data on complications was difficult to assess and was incomplete.[38] Patients with fused spines and permanent implants tend to have normal lives with unrestricted activities when they are younger; it remains to be seen whether those that have been treated with the newer surgical techniques develop problems as they age.[39]
Thoracoplasty
A complementary surgical procedure a surgeon may recommend is called thoracoplasty (also called costoplasty). This is a procedure to reduce the rib hump that affects most scoliosis patients with a thoracic curve. A rib hump is evidence of some rotational deformity to the spine. Thoracoplasty may also be performed to obtain bone grafts from the ribs instead of the pelvis, regardless of whether a rib hump is present. Thoracoplasty can be performed as part of a spinal fusion or as a separate surgery, entirely.
Thoracoplasty is the removal (or resection) of typically four to six segments of adjacent ribs that protrude. Each segment is one to two inches long. The surgeon decides which ribs to resect based on either their prominence or their likelihood to be realigned by correction of the curvature alone. The ribs grow back straight.
Thoracoplasty has risks, such as increased pain in the rib area during recovery or reduced pulmonary function (10–15% is typical) following surgery. This impairment can last anywhere from a few months to two years. Because thoracoplasty may lengthen the duration of surgery, patients may also lose more blood or develop complications from the prolonged anesthesia. A more significant, though far less common, risk is the surgeon might inadvertently puncture the pleura, a protective coating over the lungs. This could cause blood or air to drain into the chest cavity, hemothorax or pneumothorax, respectively.[40]
Surgery without fusion
New implants that aim to delay spinal fusion and to allow more spinal growth in young children have been developed. For the youngest patients, whose thoracic insufficiency compromises their ability to breathe and applies significant cardiac pressure, rib cage implants that push the ribs apart on the concave side of the curve may be especially useful. These Vertical, Expandable Prosthetic Titanium Ribs (VEPTR) provide the benefit of expanding the thoracic cavity and straightening the spine in all three dimensions while allowing it to grow.[30]
An expandable rod, called a growing rod, may be surgically implanted across the segment of spinal curvature, and lengthened, under surgery, every six months to mimic and maintain normal spine growth.[30] This intervention can halt the progress of curvature and gradually straighten the spine. A magnetically controlled growing rod (MCGR) system has been developed and is undergoing clinical trials in Hong Kong. This intervention employs a rod that may be expanded by applying strong magnets to the outside of the patient's body, and so does not involve repeated surgeries. The recently published report on the first two children to reach 24 month follow-up (aged 5 and 12 years) is encouraging. Monthly rod lengthening produced a progressive increase in spinal length and correction of scoliosis was maintained.[41][42]
Although these methods are novel and promising, they are suitable only for growing patients with early-onset scoliosis, and have a high complication rate.[30] Spinal fusion remains the "gold standard" of surgical treatment for scoliosis.[43]
Complications
The risk of undergoing surgery for scoliosis was estimated in 2008 to be varying, but with a high rate of complications. Possible complications may be inflammation of the soft tissue or deep inflammatory processes, breathing impairments, bleeding and nerve injuries. It is not yet clear what to expect from spine surgery in the long term.[44][45] Taking into account that signs and symptoms of spinal deformity cannot be changed by surgical intervention, surgery remains primarily a cosmetic indication, only especially in patients with adolescent idiopathic scoliosis, the most common form of scoliosis never exceeding 80°.[44][46] However, the cosmetic effects of surgery are not necessarily stable.[44]
For spinal fusion surgery on AIS cases, with instrumentation attached using pedicle screws, complication rates were reported in 2011 as transient neurological injuries between 0% to 1.5%, a pedicle fracture rate of 0.24%, screw malposition assessed by radiography at 1.5%, 6% when assessed by CT scans though these patients were asymptomatic not requiring screw revision, and screw loosening noted in 0.76% of patients.[30]
After-surgery care
Pain medication
In the event of surgery to correct scoliosis, pain medications and anesthesia will be administered. Before the surgery, the patient will receive anesthesia. With adults, the anesthesia will be administered through an IV in the antecubital region of the arm. With young children, however, the child will be asked to breathe in nitrous oxide, or laughing gas. Because needles can be frightening for a young child, the nitrous oxide will put them to sleep so the anesthesiologist can then insert the IV in order to give them the anesthesia. After the surgery, the patient will most likely be given morphine. Until the patient is ready to take the medicine by mouth, an IV will be giving them their medication. Morphine is the most common pain medicine used after scoliosis surgery, and is often administered through a patient-controlled analgesia (PCA) system. The PCA system allows the patient to push a button when they are feeling pain, and the PCA will emit the drugs into the IV and then into the body. To prevent overdoses, there is a limit on the number of times a patient can push the button. If a patient pushes the button too much at once, the PCA will reject the request.[47]
Bowel and bladder function
For the patient's bladder control, a catheter will be inserted so that a patient can urinate without having to move. A catheter is inserted because the patient will not have much free movement to be able to get up and walk to the bathroom. The most common type of catheter used after major surgeries is an indwelling Foley catheter. The indwelling Foley catheter is most often put in the urethra, with a tube leading into a drainage bag. Once the catheter is inserted into the urethra, a balloon is blown up inside the bladder in order to keep it from falling out. The balloon allows the catheter to remain inside the urethra until the patient is able to get up and go to the bathroom on their own.[48] The drainage bag is connected to the side of the bed, and must be changed or emptied out once it is full.
Bowel control can vary from patient to patient. The combination of no food, very little fluids, and a lot of prescription drugs has the potential to cause many patients to become constipated. The body is used to a normal diet, and used to excreting waste in a system. Interrupting the system can cause bowel problems. This constipation can be resolved in a couple of ways. The first way, and the most common way, is to administer a rectal suppository. A rectal suppository is administered through the anus, and into the rectum. They are bullet-shaped and contain medicine that will help the patient's bowels get back on track. Once the suppository is inserted, it is designed to melt off the wax-like case, and put the medicine in the body.[49] If the suppository does not work, a laxative may be continued at home to keep the bowels in full function.
Diet
When first returning home after surgery, a nutritional diet is necessary in order to keep the body operating correctly. Junk food is not a good idea, as the grease and sugar can irregulate the bowels. Fruit, vegetables, and juices will be a vital part in the diet.[50] Food and drink will be limited for the patient after surgery. Because the bowels are not fully active because of anesthetic, clear water and ice may be the only acceptable thing to ingest. After the digestive tract is back up to speed, soft food and drink like pudding, soup broth, and orange juice are acceptable.[51] Very dark urine with a strong odor means that the person is most likely dehydrated and needs more fluids. In order for the urine to become a pale or clear color, the patient will need to drink a lot of water. Juices such as prune juice are a healthy option and prune juice also helps with constipation, a common factor after surgery. When it comes to food, whole grains should be added into the diet. Whole grains can be broken down easily by the body whereas processed grains and flour cannot be broken down easily. Processed grains and flour also add to constipation.[52]
History
In 1962, Paul Harrington introduced a metal spinal system of instrumentation that assisted with straightening the spine, as well as holding it rigid while fusion took place. The original (now obsolete) Harrington rod operated on a ratchet system, attached by hooks to the spine at the top and bottom of the curvature that when cranked would distract, or straighten, the curve. The Harrington rod represented a major advance in the field, as it obviated the need for prolonged casting, allowing patients greater mobility in the postoperative period and significantly reducing the quality of life burden of fusion surgery. Additionally, as the first system to apply instrumentation directly to the spine, the Harrington rod was the precursor to most modern spinal instrumentation systems. A major shortcoming of the Harrington method was it failed to produce a posture wherein the skull would be in proper alignment with the pelvis, and it did not address rotational deformity. As a result, unfused parts of the spine would try to compensate for this in the effort to stand up straight. As the person aged, there would be increased wear and tear, early-onset arthritis, disc degeneration, muscular stiffness, and pain with eventual reliance on painkillers, further surgery, inability to work full-time, and disability. "Flatback" became the medical name for a related complication, especially for those who had lumbar scoliosis.[43]
In the 1960s, the gold standard for idiopathic scoliosis was a posterior approach using a single Harrington rod. Post-operative recovery involved bed rest, casts, and braces. Poor results became apparent over time.[53]
In the 1970s, an improved technique was developed using two rods and wires attached at each level of the spine. This segmented instrumentation system allowed patients to become mobile soon after surgery.[53]
In the 1980s, Cotrel-Dubousset instrumentation improved fixation and addressed sagittal imbalance and rotational defects unresolved by the Harrington rod system. This technique used multiple hooks with rods to give stronger fixation in three dimensions, usually eliminating the need for post-operative bracing.[53]
References
- ↑ "Treating scoliosis in children". NHS Choices. 19 February 2013. Retrieved 14 May 2014.
- ↑ "Scoliosis – Treatment in adults". NHS Choices. 19 February 2013. Retrieved 14 May 2014.
- ↑ "Idiopathic Scoliosis – Adult Nonoperative Management". Scoliosis Research Society. Retrieved 14 May 2014.
- ↑ "Idiopathic Scoliosis – Adult Surgical Treatment". Scoliosis Research Society. Retrieved 14 May 2014.
- ↑ Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M; Fusco; Minozzi; Atanasio; Zaina; Romano (2008). "Exercises reduce the progression rate of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature". Disability and Rehabilitation. 30 (10): 772–785. doi:10.1080/09638280801889568. PMID 18432435.
- ↑ DeWald, RL (2003). Spinal Deformitities: The Comprehensive Text. New York: Thieme Medical Publishers, Inc.
- ↑ Bulthuis G.J., Veldhuizen A.G., Nijenbanning G.; Veldhuizen; Nijenbanning (2008). "Clinical effect of continuous corrective force delivery in the non-operative treatment of idiopathic scoliosis: a prospective cohort study of the triac-brace". European Spine Journal. 17 (2): 231–239. doi:10.1007/s00586-007-0513-9. PMC 2226193
 . PMID 17926071.
. PMID 17926071. - 1 2 Green BN, Johson C, Moreau C.; Johnson; Moreau (2009). "Is physical activity contraindicated for individuals with scoliosis? A systematic literature review". Journal of Chiropractic Medicine. 8 (1): 25–37. doi:10.1016/j.jcm.2008.11.001. PMC 2697577. PMID 19646383.
- ↑ Paris MJ, Lang G, Benjamin MJ, Wilcox R (2008). "Standard of Care: Marfan Syndrome" (PDF). Brigham and Women's Hospital.
- ↑ Vaughn, D. and Brown, E. (2007). The Influence of an In-home Based Theraputic Exercise Program on Thoracic Kyphosis Angles. Journal of Back and Musculoskeletal Rehabilitation, 20(4), 155–165.
- ↑ Pavlu, D., Panek, D. (2009). Resistance Exercise for Prevention of Trunk Deformities. Scoliosis, 2(4),1–11.
- 1 2 3 Burd TA, Pawelek L, Lenke LG.; Pawelek; Lenke (2008). "Upper Extremity Functional Assessment After Anterior Spinal Fusion via Thoracotomy for Adolescent Idiopathic Scoliosis: Prospective Study of Twenty-Five Patients". Spine. 27 (1): 65–71. doi:10.1097/00007632-200201010-00016. PMID 11805638.
- ↑ Voda S. (2009). "Dangerous Curves: Treating adult idiopathic scoliosis". Nursing. 39 (12): 42–6. doi:10.1097/01.NURSE.0000365025.40773.4c. PMID 19934743.
- ↑ Weiss H.F. (2003). "Rehabilitation of adolescent patients with scoliosis – What do we know? A review of the literature". Pediatric Rehabilitation. 6 (3): 183–194. doi:10.1080/13638490310001636790.
- 1 2 3 Radomski, M.V. (2008). Occupational therapy for physical dysfunction sixth edition. Philadelphia: Lippincott Williams & Wilkins. p. 964. ISBN 978-0-7817-6312-7.
- 1 2 3 Rigby, P.J. (2009). Assistive technology for persons with physical disabilities: Evaluation and outcomes Thesis, Utrecht University, The Netherlands. Toronto: University of Toronto Press. ISBN 978-90-393-5041-6.
- ↑ Salter K, Jutai J, Teasell R, Foley NC, Bitensky J, Bayley M.; Jutai; Teasell; Foley; Bitensky; Bayley (2010). "Issues for selection of outcome measures in stroke rehabilitation: ICF activity". Disability and Rehabilitation. 27 (6): 315–340. doi:10.1080/09638280400008545. PMID 16040533.
- ↑ Telfer S., Solomonidis S., Spence W.; Solomonidis; Spence (2009). "An investigation of teaching staff members' and parents' views on the current state of adaptive seating technology and provision". Disability & Rehabilitation: Assistive Technology. 5 (1): 14–24. doi:10.3109/17483100903191334. PMID 19941437.
- ↑ Richardson M & Frank A.O.; Frank (2009). "Electric powered wheelchairs for those with muscular dystrophy: problems of posture, pain and deformity". Disability & Rehabilitation: Assistive Technology. 4 (3): 181–188. doi:10.1080/17483100802543114. PMID 19199130.
- ↑ Mandal A C 1996: Balanced Sitting Posture on Forward Sloping Seat
- ↑ Mandal T 2009: Better furniture types for work and studies reduces bending and pain. Association for Body Conscious Design
- ↑ Wood, Grant (2013) Published in the Academy Today (The Edge) by the American Academy of Orthosits and Prosthetist. To Brace or Not to Brace: The Three-Dimensional Nature and Growth Considerations for Adolescent Idiopathic Scoliosis, July 2013 edition pages 5 – 8,
- ↑ Negrini S, et al. Scoliosis Orthopaedic and Rehabilitation Treatment, SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. 2011. http://www.scoliosisjournal.com/content/7/1/3 . Accessed January 27, 2013.
- ↑ http://www.srs.org/patient_and_family/scoliosis/idiopathic/ adolescents/surgical_treatment.htm. Accessed January 27, 2013
- ↑ Wood, G.I. (2013), Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT): The Cheneau Brace using Rigo Principles and the Wood Cheneau Rigo (WCR) Brace. Chicago, IL.
- ↑ Herring JA (2002). Tachdjian's Pediatric Orthopaedics. Philadelphia PA: W.B. Saunders. ISBN 0-7216-5684-6.
- ↑ Weiss HR: Best Practice in conservative scoliosis care. Pflaum Company, 3rd. edition, Munich 2010
- ↑ Weiss HR, Werkmann M, Stephan C; Werkmann; Stephan (2007). "Correction effects of the ScoliOlogiC® "Chêneau light" brace in patients with scoliosis". Scoliosis. 2: 2. doi:10.1186/1748-7161-2-2. PMC 1805423. PMID 17257399.
- ↑ Weiss HR, Werkmann M, Stephan C; Werkmann; Stephan (2007). "Brace related stress in scoliosis patients – Comparison of different concepts of bracing". Scoliosis. 2: 10. doi:10.1186/1748-7161-2-10. PMC 2000861. PMID 17708766.
- 1 2 3 4 5 6 7 8 M. Stenning; I. Nelson (2011). "Recent advances in the treatment of scoliosis in children". British Editorial Society of Bone and Joint Surgery. Retrieved 1 January 2014.
- ↑ "NIH study establishes benefits of bracing in adolescents with idiopathic scoliosis". National Institutes of Health. 19 September 2013. Retrieved 8 April 2014.
- ↑ "Bracing is effective in adolescents with idiopathic scoliosis, study suggests". ScienceDaily. 19 September 2013. Retrieved 8 April 2014.
- ↑ Mehta MH (2005). "Growth as a corrective force in the early treatment of progressive infantile scoliosis". The Journal of Bone and Joint Surgery. British Volume. 87 (9): 1237–1247. doi:10.1302/0301-620X.87B9.16124. PMID 16129750.
- ↑ Infantile scoliosis outreach program: What is Mehta’s Growth Guidance Casting?
- ↑ Derotational casting for progressive infantile scoliosis, Sanders JO, D’Astous J, Fitzgerald M, Khoury JG, Kishan S, Sturm PF, J Pediatr Orthop. 2009 Sep;29(6):581-7.
- ↑ Casting and Traction Treatment Methods for Scoliosis, Jacques L. D’Astous, James O. Sanders, http://www.infantilescoliosis.org/resources/sdarticle.pdf.
- ↑ Kim YJ, Lenke LG, Kim J, et al. (2006). "Comparative analysis of pedicle screw versus hybrid instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis". Spine. 31 (3): 291–298. doi:10.1097/01.brs.0000197865.20803.d4. PMID 16449901.
- ↑ Weiss HR, Goodall D; Goodall (2008). "The treatment of adolescent idiopathic scoliosis (AIS) according to present evidence. A systematic review". European Journal of Physical and Rehabilitation Medicine. 44 (2): 177–93. PMID 18418338.
- ↑ Weill Cornell Neurological Surgery – Surgical Services. Cornellneurosurgery.org. Retrieved on 2011-01-16.
- ↑ CurvedSpine.com website. Used with permission.
- ↑ Cheung KM, Cheung JP, Samartzis D, et al. (May 2012). "Magnetically controlled growing rods for severe spinal curvature in young children: a prospective case series". Lancet. 379 (9830): 1967–74. doi:10.1016/S0140-6736(12)60112-3. PMID 22520264.
- ↑ Smith JT, Campbell RM; Campbell Jr (May 2012). "Magnetically controlled growing rods for spinal deformity". Lancet. 379 (9830): 1930–1. doi:10.1016/S0140-6736(12)60528-5. PMID 22520263.
- 1 2 Scoliosis Surgery. News-medical.net. Retrieved on 2011-01-16.
- 1 2 3 Hawes M (2006). "Impact of spine surgery on signs and symptoms of spinal deformity". Pediatric Rehabilitation. 9 (4): 318–39. doi:10.1080/13638490500402264. PMID 17111548.
- ↑ Weiss HR, Goodall D; Goodall (2008). "Rate of complications in scoliosis surgery – a systematic review of the Pub Med literature". Scoliosis. 3: 9. doi:10.1186/1748-7161-3-9. PMC 2525632. PMID 18681956.
- ↑ Hawes MC, O'Brien JP; O'Brien (2008). "A century of spine surgery: what can patients expect?". Disability and Rehabilitation. 30 (10): 808–817. doi:10.1080/09638280801889972. PMID 18432439.
- ↑ "Pain Medications After Surgery". Mayo Clinic. Retrieved 28 October 2014.
- ↑ "Urinary Catheters: Medline Plus Medical Encyclopedia". nih.gov. U.S. National Library of Medicine. Retrieved 27 October 2014.
- ↑ "Safe Use of Rectal Suppositories and Enemas in Adult Patients". Ebscohost. RCN Publishing Company.
- ↑ Love-Mignogna, Susan (May 1977). "Scoliosis". Nursing77. 7 (5): 50–55. doi:10.1097/00152193-197705000-00012.
- ↑ "Pain Medications After Surgery". About Kids Health. Retrieved 28 October 2014.
- ↑ Scoliosis (1.2 ed.). SeattleChildren.org: American Journal of Surgery. 2012. pp. 115–116.
- 1 2 3 Keith Bridwell (8 February 2013). "Idiopathic Scoliosis: Options of Fixation and Fusion of Thoracic Curves". SpineUniverse. Retrieved 21 May 2014.