Rickets
| Rickets | |
|---|---|
 | |
| Radiograph of a two-year-old rickets sufferer, with a marked genu varum (bowing of the femurs) and decreased bone opacity, suggesting poor bone mineralization | |
| Pronunciation | /ˈrɪkᵻts/ |
| Classification and external resources | |
| Specialty | Pediatrics |
| ICD-10 | E55 |
| ICD-9-CM | 268 |
| DiseasesDB | 9351 |
| MedlinePlus | 000344 |
| eMedicine | ped/2014 |
| Patient UK | Rickets |
| MeSH | D012279 |
Rickets is defective mineralization or calcification of bones before epiphyseal closure in immature mammals due to deficiency or impaired metabolism of vitamin D,[1] phosphorus or calcium,[2] potentially leading to fractures and deformity. Rickets is among the most frequent childhood diseases in many developing countries. The predominant cause is a vitamin D deficiency, but lack of adequate calcium in the diet may also lead to rickets (cases of severe diarrhea and vomiting may be the cause of the deficiency). Although it can occur in adults, the majority of cases occur in children suffering from severe malnutrition, usually resulting from famine or starvation during the early stages of childhood.
Osteomalacia is a similar condition occurring in adults, generally due to a deficiency of vitamin D but occurs after epiphyseal closure.[3]
Signs and symptoms

Signs and symptoms of rickets include:
- Bone tenderness[4]
- Dental problems[4]
- Muscle weakness (rickety myopathy)[5]
- Increased tendency for fractures (easily broken bones), especially greenstick fractures
- Skeletal deformity[4]
- Toddlers: Bowed legs and double malleoli (genu varum)[5]
- Older children: Knock-knees (genu valgum) or "windswept knees"
- Cranial deformity (such as skull bossing or delayed fontanelle closure)
- Pelvic deformity
- Pectus carinatum ("pigeon chest")
- Spinal deformity (such as kyphoscoliosis or lumbar lordosis)
- Growth disturbance
- Hypocalcemia (low level of calcium in the blood)
- Tetany (uncontrolled muscle spasms all over the body)
- Craniotabes (soft skull)
- Costochondral swelling (aka "rickety rosary" or "rachitic rosary")
- Harrison's groove[4]
- Double malleoli sign due to metaphyseal hyperplasia
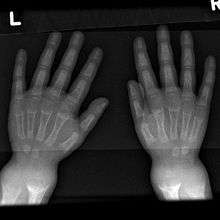
- Widening of wrist[5] raises early suspicion, it is due to metaphyseal cartilage hyperplasia.
An X-ray or radiograph of an advanced sufferer from rickets tends to present in a classic way: bow legs (outward curve of long bone of the legs) and a deformed chest. Changes in the skull also occur causing a distinctive "square headed" appearance (Caput Quadratum). These deformities persist into adult life if not treated. Long-term consequences include permanent bends or disfiguration of the long bones, and a curved back.[6]
Cause
Maternal deficiencies may be the cause of overt bone disease from before birth and impairment of bone quality after birth.[7][8] The primary cause of congenital rickets is vitamin D deficiency in the mother's blood, which the baby shares.[8] Vitamin D ensures that serum phosphate and calcium levels are sufficient to facilitate the mineralization of bone.[9] Congenital rickets may also be caused by other maternal diseases, including severe osteomalacia, untreated celiac disease, malabsorption, pre-eclampsia, and premature birth.[7] Rickets in children is similar to osteoporosis in the elderly, with brittle bones. Pre-natal care includes checking vitamin levels and ensuring that any deficiencies are supplemented.[10]
Also exclusively breast-fed infants may require rickets prevention by vitamin D supplementation or an increased exposure to sunlight.[11]
In sunny countries such as Nigeria, South Africa, and Bangladesh, there is sufficient endogenous vitamin D due to exposure to the sun. However, the disease occurs among older toddlers and children in these countries, which in these circumstances is attributed to low dietary calcium intakes due to a mainly cereal-based diet.[12]
The role of sunlight
Sunlight, especially ultraviolet light, lets human skin cells convert vitamin D from an inactive to active state. In the absence of vitamin D, dietary calcium is not properly absorbed, resulting in hypocalcaemia, leading to skeletal and dental deformities and neuromuscular symptoms, e.g. hyperexcitability. Foods that contain vitamin D include butter, eggs, fish liver oils, margarine, fortified milk and juice, portabella and shiitake mushrooms, and oily fishes such as tuna, herring, and salmon. A rare X-linked dominant form exists called vitamin D-resistant rickets or X-linked hypophosphatemia.
Cases have been reported in Britain in recent years[13] of rickets in children of many social backgrounds caused by insufficient production in the body of vitamin D because the sun's ultraviolet light was not reaching the skin due to use of strong sunblock, too much "covering up" in sunlight, or not getting out into the sun. Other cases have been reported among the children of some ethnic groups in which mothers avoid exposure to the sun for religious or cultural reasons, leading to a maternal shortage of vitamin D;[14][15] and people with darker skins need more sunlight to maintain vitamin D levels. The British Medical Journal reported in 2010 that doctors in Newcastle upon Tyne saw 20 cases of rickets per year. Rickets had been a significant malaise in London, especially during the Industrial Revolution. Persistent thick fog and heavy industrial smog permeating the city blocked out significant amounts of sunlight so much so that up to 80 percent of children at one time had varying degrees of rickets in one form or the other. Diseases causing soft bones in infants, like hypophosphatasia or hypophosphatemia can also lead to rickets.[16]
Evolutionary considerations
Vitamin D natural selection hypotheses: Rickets is often a result of Vitamin D3 deficiency. The Vitamin D natural selection hypothesis suggests that Vitamin D production from sunlight is a selective force for human skin color variation.[17][18] The correlation between human skin color and latitude is thought to be the result of positive selection to varying levels of solar ultraviolet radiation. Northern latitudes have selection for lighter skin that allows UV rays to produce Vitamin D from 7-dehydrocholesterol. Conversely, latitudes near the equator have selection for darker skin that can block the majority of UV radiation to protect from toxic levels of Vitamin D, as well as skin cancer.[19]
An anecdote often cited to support this hypothesis is that Arctic populations whose skin is relatively darker for their latitude, such as the Inuit, have a diet that is historically rich in vitamin D. Since these people acquire Vitamin D through their diet, there is not a positive selective force to synthesize Vitamin D from sunlight.[20]
Environment mismatch: Ultimately, Vitamin D deficiency arises from a mismatch between a populations previous evolutionary environment and the individual’s current environment. This risk of mismatch increases with advances in transportation methods and increases in urban population size at high latitudes.
Similar to the environmental mismatch when dark-skinned people live at high latitudes, Rickets can also occur in religious communities that require long garments with hoods and veils.[21] These hoods and veils act as sunlight barriers that prevent individuals from synthesizing Vitamin D naturally from the sun.
In a study by Mithal et al.,[22] Vitamin D insufficiency of various countries was measured by lower 25-hydroxyvitamin D. 25(OH)D is an indicator of vitamin D insufficiency that can be easily measured. These percentages should be regarded as relative Vitamin D levels, and not as predicting evidence for development of rickets.
Asian immigrants living in Europe have an increased risk for Vitamin D deficiency. Vitamin D insufficiency was found in 40% of non-Western immigrants in the Netherlands, and in more than 80% of Turkish and Moroccan immigrants.
The Middle East, despite high rates of sun-exposure, has the highest rates of rickets worldwide . This can be explained by limited sun exposure due to cultural practices and lack of vitamin D supplementation for breast-feeding women. Up to 70% and 80% of adolescent girls in Iran and Saudi Arabia, respectively, have Vitamin D insufficiency. Socioeconomic factors that limit a Vitamin D rich diet also plays a role. In the United States, Vitamin D insufficiency varies dramatically by ethnicity. Among males aged 70 years and older, the prevalence of low serum 25(OH) D levels was 23% for non-Hispanic whites, 45% for Mexican Americans, and 58% for non-Hispanic blacks. Among women, the prevalence was 28.5%, 55%, and 68%, respectively.
With this evolutionary perspective in mind, parents can supplement their nutritional intake with vitamin D enhanced beverages if they feel their child is at risk for Vitamin D deficiency,[23] or, with more assurance of benefit and no cost , enable the child to spend more time with some of their skin receiving the summer sun's rays.
Diagnosis

Rickets may be diagnosed with the help of:
- Blood tests:[24]
- Serum calcium may show low levels of calcium, serum phosphorus may be low, and serum alkaline phosphatase may be high from bones or changes in the shape or structure of the bones. This can show enlarged limbs and joints.
- Bone biopsy is rarely performed but will confirm rickets.[24]
Types
- Vitamin D-related rickets[25]
- Vitamin D deficiency
- Vitamin D-dependent rickets[25]
- Type 1 (25-Hydroxyvitamin D3 1-alpha-hydroxylase deficiency)
- Type 2 (calcitriol receptor mutation)
- Hypocalcemia-related rickets
- Hypocalcemia
- Chronic renal failure (CKD-BMD)
- Hypophosphatemia-related rickets
- Congenital
- Vitamin D-resistant rickets[25]
- Autosomal dominant hypophosphatemic rickets (ADHR)
- Autosomal recessive hypophosphatemic rickets (ARHR)[26]
- Hypophosphatemia (typically secondary to malabsorption)
- Fanconi's syndrome
- Congenital
- Secondary to other diseases
- Tumor-induced osteomalacia
- McCune-Albright syndrome
- Epidermal nevus syndrome
- Dent's disease
Differential diagnosis
Infants with rickets often have bone fractures. This sometimes leads to child abuse allegations. This issue appears to be more common for solely nursing infants of black mothers, in winter in temperate climates, suffering poor nutrition and no vitamin D supplementation.[27] People with darker skin produce less vitamin D than those with lighter skin, for the same amount of sunlight.[28]
Treatment and prevention
The most common treatment of rickets is the use of Vitamin D.[29] However, surgery may be required to remove severe bone abnormalities.[25]
Diet and sunlight
Treatment involves increasing dietary intake of calcium, phosphates and vitamin D. Exposure to ultraviolet B light (most easily obtained when the sun is highest in the sky), cod liver oil, halibut-liver oil, and viosterol are all sources of vitamin D.
A sufficient amount of ultraviolet B light in sunlight each day and adequate supplies of calcium and phosphorus in the diet can prevent rickets. Darker-skinned people need to be exposed longer to the ultraviolet rays. The replacement of vitamin D has been proven to correct rickets using these methods of ultraviolet light therapy and medicine.[30]
Recommendations are for 400 international units (IU) of vitamin D a day for infants and children. Children who do not get adequate amounts of vitamin D are at increased risk of rickets. Vitamin D is essential for allowing the body to uptake calcium for use in proper bone calcification and maintenance.
Supplementation
Sufficient vitamin D levels can also be achieved through dietary supplementation and/or exposure to sunlight. Vitamin D3 (cholecalciferol) is the preferred form since it is more readily absorbed than vitamin D2. Most dermatologists recommend vitamin D supplementation as an alternative to unprotected ultraviolet exposure due to the increased risk of skin cancer associated with sun exposure. Endogenous production with full body exposure to sunlight is approximately 250 µg (10,000 IU) per day.[31]
According to the American Academy of Pediatrics (AAP), all infants, including those who are exclusively breast-fed, may need Vitamin D supplementation until they start drinking at least 17 US fluid ounces (500 ml) of vitamin D-fortified milk or formula a day.[32]
Epidemiology
In developed countries, rickets is a rare disease[33] (incidence of less than 1 in 200,000). Recently, cases of rickets have been reported among children who are fed plant-based milk substitutes and not given supplemental vitamin D.[34]
Those at higher risk for developing rickets include:
- Breast-fed infants whose mothers are not exposed to sunlight
- Breast-fed infants who are not exposed to sunlight
- Breast-fed babies who are exposed to little sunlight
- Adolescents, in particular when undergoing the pubertal growth spurt[35]
- Any child whose diet does not contain enough vitamin D or calcium
History
Greek physician Soranus of Ephesus, one of the chief representatives of the Methodic school of medicine who practiced in Alexandria and subsequently in Rome, reported deformation of the bones in infants as early as the first and second centuries AD. Rickets was not defined as a specific medical condition until 1645, when an English physician Daniel Whistler gave the earliest known description of the disease. In 1650 a treatise on rickets was published by Francis Glisson, a physician at Caius College, Cambridge,[36] who said it had first appeared about 30 years previously in the counties of Dorset and Somerset.[37] In 1857, John Snow suggested rickets, then widespread in Britain, was being caused by the adulteration of bakers' bread with alum.[38] German pediatrician Kurt Huldschinsky successfully demonstrated in the winter of 1918–1919 how rickets could be treated with ultraviolet lamps. The role of diet in the development of rickets[39][40] was determined by Edward Mellanby between 1918–1920.[41] In 1923, American physician Harry Steenbock demonstrated that irradiation by ultraviolet light increased the vitamin D content of foods and other organic materials. Steenbock's irradiation technique was used for food stuffs, but most memorably for milk. By 1945, rickets had all but been eliminated in the United States, no cases have been recorded in Cuba, but they are there since the Special Period.
Etymology
The word rickets may be from the Old English word wrickken ('to twist'), although because this is conjectured, several major dictionaries simply say "origin unknown". The name rickets is plural in form but usually singular in construction. The Greek word "rachitis" (ῥαχίτης,[42] meaning "in or of the spine") was later adopted as the scientific term for rickets, due chiefly to the words' similarity in sound.
See also
Notes
References
- ↑ Magnesium and vitamin D's co-factors, by John Jacob Cannell, M.D. citing The Lancet; The Vitamin D Council "Two interesting cases of Mg dependent Vitamin D-resistant rickets appeared in the Lancet in 1974. Two children, one age two and the other age five, presented with classic rickets. 600,000 IU of Vitamin D daily for ten days did not result in any improvement in six weeks—in either x-rays or alkaline phosphatase—and the doctors diagnosed Vitamin D-resistant rickets. Almost by accident, serum Mg levels were then obtained, which were low in both children. After the treatment with Mg, the rickets rapidly resolved."
- ↑ TheFreeDictionary > rickets In turn citing:
- The American Heritage Medical Dictionary Copyright 2007 (mentioning vitamin D and phosphates)
- Mosby's Dental Dictionary, 2nd edition. Copyright 2008 (mentioning vitamin D and calcium)
- ↑ MedlinePlus Medical Encyclopedia: Osteomalacia
- 1 2 3 4 Medical News – Symptoms of Rickets
- 1 2 3 Mayo Clinic – Signs and Symptoms of Rickets
- ↑ Pharmacologyonline. "Rickets and its Management: A Review" (PDF). Retrieved 2 June 2012.
- 1 2 Elidrissy AT (2016). "The Return of Congenital Rickets, Are We Missing Occult Cases?". Calcif Tissue Int (Review). 99 (3): 227–36. doi:10.1007/s00223-016-0146-2. PMID 27245342.
- 1 2 Paterson CR, Ayoub D (2015). "Congenital rickets due to vitamin D deficiency in the mothers.". Clin Nutr (Review). 34 (5): 793–8. doi:10.1016/j.clnu.2014.12.006. PMID 25552383.
- ↑ https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
- ↑ http://www.webmd.com/baby/guide/prenatal-vitamins#1
- ↑ Balasubramanian S, Ganesh R (2008). "Vitamin D deficiency in exclusively breast-fed infants". The Indian Journal of Medical Research (Review). 127 (3): 250–5. PMID 18497439.
- ↑ Pettifor JM (2004). "Nutritional rickets: deficiency of vitamin D, calcium, or both?". The American Journal of Clinical Nutrition (Review). 80 (6 Suppl): 1725S–9S. PMID 15585795.
- ↑ Daily Telegraph, page 4, Wednesday 19 January 2011
- ↑ Rise in rickets linked to ethnic groups that shun the sun The Independent, published 2011-07-25, accessed 2011-07-251
- ↑ Doctors fear rickets resurgence BBC, published 2007-12-28, accessed 2011-07-25
- ↑ "Hypophosphatasia: Signs and Symptoms". Hypophosphatasia.com. Retrieved 10 September 2014.
- ↑ Yuen, A.W.C.; Jablonski, N.G. (January 2010). "Vitamin D: In the evolution of human skin colour". Medical Hypotheses. 74 (1): 39–44. doi:10.1016/j.mehy.2009.08.007. PMID 19717244.
- ↑ Murray, F.G. (July–September 1934). "Pigmentation, Sunlight, and Nutritional Disease". American Anthropologist. 36 (3): 438–445. doi:10.1525/aa.1934.36.3.02a00100.
- ↑ Loomis, W.G. (August 1967). "Skin-pigment regulation of vitamin-D biosynthesis in man". Science. 157 (3788): 501–6. doi:10.1126/science.157.3788.501. PMID 6028915.
- ↑ Barr, Sharma; Macdonald H.M., Sheehy T., Novotny R., Corriveau A. (August 2011). "Vitamin D deficiency and disease risk among aboriginal Arctic populations". Nutritional Review. 69 (8): 468–478. doi:10.1111/j.1753-4887.2011.00406.x.
- ↑ Bachrach, S.; Fisher J., Parks J.S. (1979). "An outbreak of vitamin D deficiency rickets in a susceptible population". Pediatrics Volume. 64 (6): 871–877.
- ↑ Mithal, A.; Wahl D.A., Bonjour J.P., Burckhardt T., Dawson-Hughes B., Eisman J.A., El-Hajj Fuleihan G., Josse R.G., Lips P., Morales-Torres J. (19 June 2009). "Global vitamin D status and determinants of hypovitaminosis D". Osteoporosis International. 20: 1807–1820. doi:10.1007/s00198-009-0954-6.
- ↑ Weisberg, P.; Scanlon K.S., Ruowei L., Cogswell M.E. (2004). "Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003". The American Journal of Clinical Nutrition. 80 (6): 1697S–1705S.
- 1 2 NHS Choice - Rickets Diagnoses
- 1 2 3 4 Rickets: Not a Disease of the Past
- ↑ Autosomal-recessive hypophosphatemic rickets is associated with an inactivation mutation in the ENPP1 gene.
- ↑ Keller, Kathy A.; Barnes, Patrick D. (22 September 2008). "Rickets vs. abuse: a national and international epidemic" (PDF). Pediatric Radiology. 38 (11): 1210–1216. doi:10.1007/s00247-008-1001-z. PMID 18810424.
- ↑ Live Strong. "CDark Skin Color & Vitamin D". Retrieved 2 June 2012.
- ↑ Meschino Health. "Complete Guide to Vitamin D". Retrieved 2 June 2012.
- ↑ Rajakumar, Kumaravel (1 August 2003). "Vitamin D, Cod-Liver Oil, Sunlight, and Rickets: A Historical Perspective". Pediatrics. 112 (2): e132–e135. doi:10.1542/peds.112.2.e132. PMID 12897318. Retrieved 14 July 2011.
- ↑ Vieth R (May 1999). "Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety". The American Journal of Clinical Nutrition. 69 (5): 842–56. PMID 10232622.
- ↑ Gartner LM, Greer FR (April 2003). "Prevention of rickets and vitamin D deficiency: new guidelines for vitamin D intake". Pediatrics. 111 (4 Pt 1): 908–10. doi:10.1542/peds.111.4.908. PMID 12671133.
- ↑ National Health Service of England > Rickets Last reviewed: 28 January 2010
- ↑ http://www.stmichaelshospital.com/media/detail.php?source=hospital_news/2014/20141020_hn
- ↑ Glorieux FH, Pettifor JM (2014). "Vitamin D/dietary calcium deficiency rickets and pseudo-vitamin D deficiency rickets". BoneKEy Reports (Review). 3: 524. doi:10.1038/bonekey.2014.19. PMC 4015456
 . PMID 24818008.
. PMID 24818008. - ↑ Claerr, Jennifer (February 6, 2008). "The History of Rickets, Scurvy and Other Nutritional Deficiencies". An Interesting Treatise on Human Stupidity. Yahoo! Voices. Archived from the original on 2013-03-26.
URL references
- ↑ Gibbs D (1994). "Rickets and the crippled child: an historical perspective". Journal of the Royal Society of Medicine. 87 (12): 729–32. PMC 1294978. PMID 7503834.
- ↑ Dunnigan M (2003). "Commentary: John Snow and alum-induced rickets from adulterated London bread: an overlooked contribution to metabolic bone disease". International Journal of Epidemiology. 32 (3): 340–1. doi:10.1093/ije/dyg160. PMID 12777415.
- ↑ Pileggi VJ, De Luca HF, Steenbock H (September 1955). "The role of vitamin D and intestinal phytase in the prevention of rickets in rats on cereal diets". Archives of Biochemistry and Biophysics. 58 (1): 194–204. doi:10.1016/0003-9861(55)90106-5. PMID 13259690.
- ↑ Ford JA, Colhoun EM, McIntosh WB, Dunnigan MG (1972). "Biochemical Response of Late Rickets and Osteomalacia to a Chupatty-free Diet". British Medical Journal. 3 (5824): 446–7. doi:10.1136/bmj.3.5824.446. PMC 1786011. PMID 5069221.
- ↑ Rajakumar K (2003). "Vitamin D, cod-liver oil, sunlight, and rickets: a historical perspective". Pediatrics. 112 (2): e132–5. doi:10.1542/peds.112.2.e132. PMID 12897318.
- ↑ Greek Word Study Tool