Streptococcus
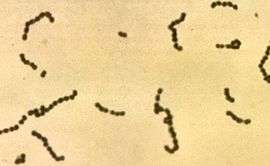
Streptococcus is a genus of coccus (spherical) Gram-positive bacteria belonging to the phylum Firmicutes[3] and the order Lactobacillales (lactic acid bacteria). Cell division in this genus occurs along a single axis in these bacteria, thus they grow in chains or pairs, hence the name—from Greek στρεπτός streptos, meaning easily bent or twisted, like a chain (twisted chain). (Contrast this with staphylococci, which divide along multiple axes and generate grape-like clusters of cells.)
Most are oxidase-negative and catalase-negative, and many are facultative anaerobes.
In 1984, many bacteria formerly considered Streptococcus were separated out into the genera Enterococcus and Lactococcus.[4] Currently, over 50 species are recognised in this genus.
Pathogenesis and classification
In addition to streptococcal pharyngitis (strep throat), certain Streptococcus species are responsible for many cases of pink eye,[5] meningitis, bacterial pneumonia, endocarditis, erysipelas, and necrotizing fasciitis (the 'flesh-eating' bacterial infections). However, many streptococcal species are not pathogenic, and form part of the commensal human microbiota of the mouth, skin, intestine, and upper respiratory tract. Furthermore, streptococci are a necessary ingredient in producing Emmentaler ("Swiss") cheese.
Species of Streptococcus are classified based on their hemolytic properties.[6] Alpha-hemolytic species cause oxidization of iron in hemoglobin molecules within red blood cells, giving it a greenish color on blood agar. Beta-hemolytic species cause complete rupture of red blood cells. On blood agar, this appears as wide areas clear of blood cells surrounding bacterial colonies. Gamma-hemolytic species cause no hemolysis.
Beta-hemolytic streptococci are further classified by Lancefield grouping, a serotype classification (that is, describing specific carbohydrates present on the bacterial cell wall).[7] The 20 described serotypes are named Lancefield groups A to V (excluding I and J).
In the medical setting, the most important groups are the alpha-hemolytic streptococci S. pneumoniae and Streptococcus viridans group, and the beta-hemolytic streptococci of Lancefield groups A and B (also known as “group A strep” and “group B strep”).
Table: Medically relevant streptococci (not all are alpha hemolytic)[6]
| Species | Host | Disease |
| S. pyogenes | human | pharyngitis |
| S. agalactiae | human, cattle | neonatal meningitis and sepsis |
| S. dysgalactiae | human, animals | endocarditis, bacteremia, pneumonia, meningitis, respiratory infections |
| S. bovis | human, animals | biliary or urinary tract infections, endocarditis |
| S. anginosus | human, animals | subcutaneous/organ abscesses, meningitis, respiratory infections |
| S. sanguinis | human | endocarditis, dental caries |
| S. suis | swine | meningitis |
| S. mitis | human | endocarditis |
| S. mutans | human | dental caries |
| S. pneumoniae | human | pneumonia |
Alpha-hemolytic
When alpha hemolysis (α-hemolysis) is present, the agar under the colony is dark and greenish. Streptococcus pneumoniae and a group of oral streptococci (Streptococcus viridans or viridans streptococci) display alpha hemolysis. This is sometimes called green hemolysis because of the color change in the agar. Other synonymous terms are incomplete hemolysis and partial hemolysis. Alpha hemolysis is caused by hydrogen peroxide produced by the bacterium, oxidizing hemoglobin to green methemoglobin.
Pneumococci
- S. pneumoniae (sometimes called pneumococcus), is a leading cause of bacterial pneumonia and occasional etiology of otitis media, sinusitis, meningitis, and peritonitis. Inflammation is thought to be the major cause of how pneumococci cause disease, hence the tendency of diagnoses associated with them to involve inflammation.
The viridans group: alpha-hemolytic
- The viridans streptococci are a large group of commensal bacteria, that are either α-hemolytic, producing a green coloration on blood agar plates (hence the name "viridans", from Latin vĭrĭdis, green), or nonhemolytic. They possess no Lancefield antigens.[3]
Beta-hemolytic
Beta hemolysis (β-hemolysis), sometimes called complete hemolysis, is a complete lysis of red cells in the media around and under the colonies: the area appears lightened (yellow) and transparent. Streptolysin, an exotoxin, is the enzyme produced by the bacteria which causes the complete lysis of red blood cells. There are two types of streptolysin: Streptolysin O (SLO) and streptolysin S (SLS). Streptolysin O is an oxygen-sensitive cytotoxin, secreted by most Group A streptococcus (GAS), and interacts with cholesterol in the membrane of eukaryotic cells (mainly red and white blood cells, macrophages, and platelets), and usually results in β-hemolysis under the surface of blood agar. Streptolysin S is an oxygen-stable cytotoxin also produced by most GAS strains which results in clearing on the surface of blood agar. SLS affects immune cells, including polymorphonuclear leukocytes and lymphocytes, and is thought to prevent the host immune system from clearing infection. Streptococcus pyogenes, or group A Streptococcus (GAS), displays beta hemolysis.
Some weakly beta-hemolytic species cause intense beta hemolysis when grown together with a strain of Staphylococcus. This is called the CAMP test. Streptococcus agalactiae displays this property. Clostridium perfringens can be identified presumptively with this test. Listeria monocytogenes is also positive on sheep's blood agar.

Group A
S. pyogenes (GAS) is the causative agent in a wide range of group A streptococcal infections. These infections may be noninvasive or invasive. The noninvasive infections tend to be more common and less severe. The most common of these infections include streptococcal pharyngitis (strep throat) and impetigo.[8] Scarlet fever is also a noninvasive infection, but has not been as common in recent years.
The invasive infections caused by group A β-hemolytic streptococci tend to be more severe and less common. This occurs when the bacterium is able to infect areas where it is not usually found, such as the blood and the organs.[9] The diseases that may be caused include streptococcal toxic shock syndrome, necrotizing fasciitis, pneumonia, and bacteremia.[8] Globally, GAS has been estimated to cause more than 500,000 deaths every year, making it one of the world's leading pathogens.[8]
Additional complications may be caused by GAS, namely acute rheumatic fever and acute glomerulonephritis. Rheumatic fever, a disease that affects the joints, kidneys, and heart valves, is a consequence of untreated strep A infection caused not by the bacterium itself. Rheumatic fever is caused by the antibodies created by the immune system to fight off the infection cross-reacting with other proteins in the body. This "cross-reaction" causes the body to essentially attack itself and leads to the damage above. A similar autoimmune mechanism initiated by Group A beta-hemolytic streptococcal (GABHS) infection is hypothesized to cause pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS), wherein autoimmune antibodies affect the basal ganglia, causing rapid onset of psychiatric, motor, sleep, and other symptoms in pediatric patients.
Group A Streptococcus infection is generally diagnosed with a rapid strep test or by culture.
Group B
S. agalactiae, or group B Streptococcus, GBS, causes pneumonia and meningitis in neonates and the elderly, with occasional systemic bacteremia. They can also colonize the intestines and the female reproductive tract, increasing the risk for premature rupture of membranes during pregnancy, and transmission of the organism to the infant. The American Congress of Obstetricians and Gynecologists (formerly the American College of Obstetricians and Gynecologists), American Academy of Pediatrics, and the Centers for Disease Control recommend all pregnant women between 35 and 37 weeks gestation to be tested for GBS. Women who test positive should be given prophylactic antibiotics during labor, which will usually prevent transmission to the infant.[10]
The United Kingdom has chosen to adopt a risk factor-based protocol, rather than the culture-based protocol followed in the US. Current guidelines state that if one or more of the following risk factors are present, then women should be treated with intrapartum antibiotics:
- Preterm labour (<37 weeks)
- Prolonged rupture of membranes (>18 hours)
- Intrapartum fever (>38C)
- Prior GBS affected infant
- GBS bacteriuria during this pregnancy
This protocol results in treatment of 15–20% of pregnant women and prevention of 65–70% of cases of early onset GBS sepsis.[11]
Group C
This group includes S. equi, which causes strangles in horses,[12] and S. zooepidemicus—S. equi is a clonal descendent or biovar of the ancestral S. zooepidemicus—which causes infections in several species of mammals, including cattle and horses. S. dysgalactiae is also a member of group C, β-haemolytic streptococci that can cause pharyngitis and other pyogenic infections similar to group A streptococci.
Group D (enterococci)
Many former group D streptococci have been reclassified and placed in the genus Enterococcus (including E. faecalis, E. faecium, E. durans, and E. avium).[13] For example, Streptococcus faecalis is now Enterococcus faecalis. E. faecalis is sometimes alpha hemolytic and E. faecium is sometimes beta hemolytic.[14]
The remaining nonenterococcal group D strains include Streptococcus bovis and Streptococcus equinus.
Nonhemolytic streptococci rarely cause illness. However, weakly hemolytic group D beta-hemolytic streptococci and Listeria monocytogenes (which is actually a Gram-positive bacillus) should not be confused with nonhemolytic streptococci.
Group F streptococci
Group F streptococci were first described in 1934 by Long and Bliss amongst the "minute haemolytic streptococci".[15] They are also known as Streptococcus anginosus (according to the Lancefield classification system) or as members of the S. milleri group (according to the European system).
Group G streptococci
These streptococci are usually, but not exclusively, beta-hemolytic. Streptococcus dysgalactiae is the predominant species encountered, particularly in human disease. S. canis is an example of a GGS which is typically found on animals, but can cause infection in humans. S. phocae is a GGS subspecies that has been found in marine mammals and marine fish species. In marine mammals it has been mainly associated with meningoencephalitis, septicemia, and endocarditis, but is also associated with many other pathologies. It's environmental reservoir and means of transmission in marine mammals is not well characterized.
Group H streptococci
Group H streptococci cause infections in medium-sized canines. Group H streptococci rarely cause illness unless a human has direct contact with the mouth of a canine. One of the most common ways this can be spread is human-to-canine, mouth-to-mouth contact. However, the canine may lick the human's hand and infection can be spread, as well.[16]
Molecular taxonomy and phylogenetics
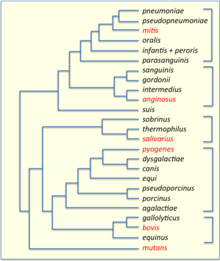
Streptococci have been divided into six groups on the basis of their 16S rDNA sequences: S. anginosus, S.bovis, S. mitis, S. mutans, S. pyogenes and S. salivarius.[18] The 16S groups have been confirmed by whole genome sequencing (see figure). The important pathogens S. pneumoniae and S. pyogenes belong to the S. mitis and S. pyogenes groups, respectively, while the causative agent of dental caries, Streptococcus mutans, is basal to the Streptococcus group.
Genomics
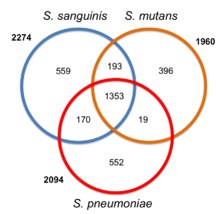
The genomes of hundreds of species have been sequenced.[20] Most Streptococcus genomes are 1.8 to 2.3 Mb in size and encode 1,700 to 2,300 proteins. Some important genomes are listed in the table.[21] The four species shown in the table (S. pyogenes, S. agalactiae, S. pneumoniae, and S. mutans) have an average pairwise protein sequence identity of about 70%.[21]
| feature | S. pyogenes | S. agalactiae | S. pneumoniae | S. mutans |
|---|---|---|---|---|
| base pairs | 1,852,442 | 2,211,488 | 2,160,837 | 2,030,921 |
| ORFs | 1792 | 2118 | 2236 | 1963 |
| prophages | yes | no | no | no |
Bacteriophage
Bacteriophages have been described for many species of Streptococcus. 18 prophages have been described in S. pneumoniae that range in size from 38 to 41 kb in size, encoding from 42 to 66 genes each. Some of the first Streptococcus phages discovered were Dp-1[22] and ω1.[23][24] In 1981 the Cp (Complutense phage) family was discovered with Cp-1 as its first member.[25] Dp-1 and Cp-1 infect both S. pneumoniae and S. mitis.[26] However, the host ranges of most Streptococcus phages have not been investigated systematically.
See also
References
- ↑ "Result of detail taxonomy information". TXSearch Taxonomy Retrieval. DNA Data Bank of Japan. 19 February 2010. Retrieved 30 March 2010.
- ↑ LPSN entry for Streptococcus
- 1 2 Ryan KJ, Ray CG, eds. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 293–4. ISBN 0-8385-8529-9.
- ↑ Facklam R (October 2002). "What happened to the streptococci: overview of taxonomic and nomenclature changes". Clin. Microbiol. Rev. 15 (4): 613–30. doi:10.1128/CMR.15.4.613-630.2002. PMC 126867
 . PMID 12364372.
. PMID 12364372. - ↑ http://www.medicinenet.com/pink_eye/article.htm
- 1 2 Patterson MJ (1996). Baron S; et al., eds. Streptococcus. In: Baron's Medical Microbiology (4th ed.). Univ of Texas Medical Branch. (via NCBI Bookshelf) ISBN 0-9631172-1-1.
- ↑ Facklam R (2002). "What happened to the streptococci: overview of taxonomic and nomenclature changes". Clin Microbiol Rev. 15 (4): 613–30. doi:10.1128/CMR.15.4.613-630.2002. PMC 126867. PMID 12364372.
- 1 2 3 Cohen-Poradosu R, Kasper DL (2007). "Group A streptococcus epidemiology and vaccine implications". Clin. Infect. Dis. 45 (7): 863–5. doi:10.1086/521263. PMID 17806050.
- ↑ "Streptococcal Infections (Invasive Group A Strep)". New York City Department of Health and Mental Hygiene. Retrieved 21 November 2012.
- ↑ Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A (2002). "Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC". MMWR Recomm Rep. 51 (RR-11): 1–22. PMID 12211284.
- ↑ Norwitz, E.R.; Schorge, J.O. (2013). Obstetrics and Gynaecology at a Glance (4th ed.). John Wiley & Sons LTD.
- ↑ Harrington DJ, Sutcliffe IC, Chanter N (2002). "The molecular basis of Streptococcus equi infection and disease". Microbes Infect. 4 (4): 501–10. doi:10.1016/S1286-4579(02)01565-4. PMID 11932201.
- ↑ Köhler W (June 2007). "The present state of species within the genera Streptococcus and Enterococcus". International Journal of Medical Microbiology. 297 (3): 133–50. doi:10.1016/j.ijmm.2006.11.008. PMID 17400023.
- ↑ Holt et al. (1994). Bergey's Manual of Determinative Bacteriology (9th ed.). Lippincott Williams & Wilkins. ISBN 0-683-00603-7
- ↑ Whitworth JM (November 1990). "Lancefield group F and related streptococci" (PDF). J. Med. Microbiol. 33 (3): 135–51. doi:10.1099/00222615-33-3-135. PMID 2250284.
- ↑ "Bacterial Infection (Streptococcus) in Dogs". petmd.com. Retrieved 12 December 2014.
- ↑ "Bacteria-Firmicutes-Bacilli-Lactobacillales-Streptococcaceae-Streptococcus". PATRIC, University of Chicago. Retrieved 12 December 2014.
- ↑ Kawamura Y, Hou XG, Sultana F, Miura H, Ezaki T (1995). "Determination of 16S rRNA sequences of Streptococcus mitis and Streptococcus gordonii and phylogenetic relationships among members of the genus Streptococcus". Int J Syst Bacteriol. 45: 406–408. doi:10.1099/00207713-45-2-406. PMID 7537076.
- ↑ Xu, P; Alves, J. M.; Kitten, T; Brown, A; Chen, Z; Ozaki, L. S.; Manque, P; Ge, X; Serrano, M. G.; Puiu, D; Hendricks, S; Wang, Y; Chaplin, M. D.; Akan, D; Paik, S; Peterson, D. L.; MacRina, F. L.; Buck, G. A. (2007). "Genome of the opportunistic pathogen Streptococcus sanguinis". Journal of Bacteriology. 189 (8): 3166–75. doi:10.1128/JB.01808-06. PMC 1855836. PMID 17277061.
- ↑ Streptococcus genomes and related information at PATRIC
- 1 2 Ferretti JJ, Ajdic D, McShan WM (2004). "Comparative genomics of streptococcal species". The Indian journal of medical research. 119 Suppl: 1–6. PMID 15232152.
- ↑ McDonnell M, Ronda C, Tomasz A (1975) “Diplophage”: a bacteriophage of Diplococcus pneumoniae. Virology 63:577–582
- ↑ Tiraby JG, Tiraby E, Fox MS (1975) Pneumococcal bacteriophages. Virology 68:566–569
- ↑ López R (2004). "Streptococcus pneumoniae and its bacteriophages: one long argument". Int. Microbiol. 7 (3): 163–71. PMID 15492930.
- ↑ Ronda C, López R, García E (1981). "Isolation and characterization of a new bacteriophage, Cp-1, infecting Streptococcus pneumoniae". J. Virol. 40 (2): 551–9. PMC 256658. PMID 6275103.
- ↑ Ouennane S, Leprohon P, Moineau S (2015). "Diverse virulent pneumophages infect Streptococcus mitis". PLoS ONE. 10 (2): e0118807. doi:10.1371/journal.pone.0118807. PMC 4334900. PMID 25692983.
External links
- Streptococcus genomes and related information at PATRIC, a Bioinformatics Resource Center funded by NIAID
- "Adoption of perinatal group B streptococcal disease prevention recommendations by prenatal-care providers—Connecticut and Minnesota, 1998". MMWR Morb. Mortal. Wkly. Rep. 49 (11): 228–32. March 2000. PMID 10763673.
- The Canadian Strep B Foundation
- The UK Group B Strep Support charity