Tonsillectomy
| Tonsillectomy | |
|---|---|
| Intervention | |
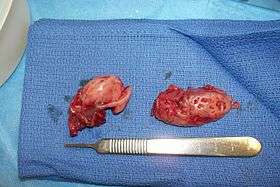 Cryptic tonsils immediately following surgical removal (bilateral tonsillectomy). | |
| ICD-9-CM | 28.2-28.3 |
| MeSH | D014068 |
| MedlinePlus | 003013 |
Tonsillectomy is a surgical procedure in which each tonsil is removed from a recess in the side of the pharynx called the tonsillar fossa. The procedure is performed in response to repeated occurrence of acute tonsillitis, sleep surgery for obstructive sleep apnea, nasal airway obstruction, diphtheria carrier state, snoring, or peritonsillar abscess. For children, the adenoids (also known as a pharyngeal tonsil or nasopharyngeal tonsil) are usually removed, a procedure called adenoidectomy (or tonsilloadenoidectomy or adenotonsillectomy when combined). Adenoidectomy is uncommon in adults in whom the adenoids are usually vestigial. Although tonsillectomy is performed less frequently than in the 1950s, it remains one of the most common surgical procedures in children in the United States.
Medical uses

Tonsillectomy may be indicated when the patient experiences recurrent infections of acute tonsillitis. As the size of tonsils reaches its maximum at 3 years of age and then regresses gradually, tonsillectomy is usually delayed unless the frequency of infection necessitates it absolutely. The number prompting tonsillectomy varies with the severity of the episodes. One case, even severe, is generally not enough for most surgeons to decide tonsillectomy is necessary. Paradise in 1983 defined recurrent tonsillitis warranting surgery by the attack frequency standard as
"Seven or more in a year, five or more per year for two years, or three or more per year for three years. These are the absolute indications for tonsillectomy."[1]
According to the 2012 guidelines of the American Academy of Otolaryngology & Head and Neck Surgery (AAO-HNS), tonsillectomy is indicated as follows:
"Clinicians may recommend tonsillectomy for recurrent throat infection with a frequency of at least 7 episodes in the past year or at least 5 episodes per year for 2 years or at least 3 episodes per year for 3 years with documentation in the medical record for each episode of sore throat and one or more of the following: temperature >38.3 °C, cervical adenopathy, tonsillar exudates, or positive test for Group A Beta- hemolytic strep."[2]
Tonsillectomy is also sometimes performed on those who suffer chronically from tonsilloliths.[3]
Most recently, American Academy of Otolaryngology-Head and Neck Surgery Foundation has published clinical practice guidelines.[4][5] The panel made a strong recommendation for:
- Watchful waiting for recurrent throat infection if there have been fewer than 7 episodes in the past year or fewer than 5 episodes per year in the past 2 years or fewer than 3 episodes per year in the past 3 years;
- Assessing the child with recurrent throat infection who does not meet criteria in statement 2 for modifying factors that may nonetheless favor tonsillectomy, which may include but are not limited to multiple antibiotic allergy/intolerance, periodic fever, aphthous stomatitis, pharyngitis and adenitis, or history of peritonsillar abscess;
- Asking caregivers of children with sleep-disordered breathing and tonsil hypertrophy about comorbid conditions that might improve after tonsillectomy, including growth retardation, poor school performance, enuresis, and behavioral problems;
- Counseling caregivers about tonsillectomy as a means to improve health in children with abnormal polysomnography who also have tonsil hypertrophy and sleep-disordered breathing;
- Counseling caregivers that sleep-disordered breathing may persist or recur after tonsillectomy and may require further management;
- Advocating for pain management after tonsillectomy and educating caregivers about the importance of managing and reassessing pain; and
- Clinicians who perform tonsillectomy should determine their rate of primary and secondary posttonsillectomy hemorrhage at least annually.
Effectiveness
The scientific evidence indicates that tonsillectomy is on average only modestly effective at reducing the frequency and severity of sore throats, and does not get rid of sore throats altogether.[6][7][8]
This raises questions about which children benefit enough to justify undertaking the operation. In children who meet strict criteria indicating that they are severely affected by sore throats, the evidence indicates that there is a short term benefit.[9]
The strict criteria are that children should have experienced 7 documented sore throats in the previous year, or 5 each year in the two previous years, or 3 each year in the three previous years and that those documented sore throats should in addition either have documented evidence of enlarged lymph glands, raised temperature, positive throat swabs (demonstrating Streptococcal infection) or pus seen on the tonsils. Children with undocumented sore throats or sore throats that are not as severe do not appear to suffer from as many sore throats in subsequent years and therefore tonsillectomy is not worthwhile.[8][10]
In children meeting the strict criteria for surgery, short term benefit means that without tonsillectomy a child who meets these strict criteria will probably have 6 sore throats in the next two years while one who has surgery will probably have 3 sore throats. After two years there is little difference in the frequency of sore throats.[11]
Given that children must have many documented sore throats for tonsillectomy to be worthwhile there is surprisingly little published evidence about how many children who have their tonsils removed actually meet these criteria. One small study in the UK demonstrated that most children who had their tonsils removed did not meet these criteria, meaning that most children operated on did not really benefit from the procedure.[12]
Criteria for tonsillectomy in children
Seven documented sore throats in the previous year, or five documented sore throats each year in the two previous years, or three documented sore throats each year in the three previous years
Sore throats should in addition either have documented evidence of enlarged lymph glands, raised temperature, positive throat swabs (demonstrating Streptococcal infection) or pus seen on the tonsils.
Children with undocumented sore throats or sore throats that are not as severe do not appear to suffer from as many sore throats in subsequent years and therefore tonsillectomy is not worthwhile.
Please note that the term "sore throat" is preferred to "throat infection" or "tonsillitis" because without undertaking throat swabs doctors cannot reliably distinguish between sore throats caused by infection and those due to other causes. The same patient may be described as suffering from tonsillitis or sore throat (pharyngitis) by different doctors, therefore the use of one term rather than the other is as dependent on the doctor as well as the patient, making it an unreliable reason for undertaking surgery.
Complications
A single dose of the corticosteroid drug dexamethasone may be given during surgery to prevent post-operative vomiting.[13] A systematic review found that a dose of dexamethasone during surgery can prevent vomiting in one out of every five children who receives the drug.[13] The review also found that these children return to a normal diet more quickly and have less post-operative pain.[13]
A recent study states that tonsillectomies in young children (0 to 7 years) are correlated with weight gain in the years following surgery.[14] However, no causal effect has been established.[15]
The morbidity rate associated with tonsillectomy is 2% to 4% due to post-operative bleeding; the mortality rate is 1 in 15,000, due to bleeding, airway obstruction, or anesthesia complications.[16]
Surgical procedure
For the past 50 years at least, tonsillectomy has been performed by dissecting the tonsil from its surrounding fascia, a so-called 'total', or extra-capsular tonsillectomy. Problems including pain and bleeding led to a recent resurgence in interest in sub-total tonsillectomy or 'tonsillotomy' which was popular 60–100 years ago, in an effort to reduce these complications.[17] The generally accepted procedure for 'total' tonsillectomy uses a scalpel and blunt dissection or electrocautery, although harmonic scalpels or lasers have also been used. Bleeding is stopped with electrocautery, ligation by sutures, and the topical use of thrombin, a protein that induces blood clotting.
The main question of importance becomes whether or not the benefits of subtotal tonsillectomy in obstructive sleep apnea are enduring. It appears that this may be the case although most observers agree that further time and study is required.[18]
Methods
The scalpel is the preferred surgical instrument of many ear, nose, and throat specialists. However, there are other techniques and a brief review of each follows:
- Dissection and snare method: Removal of the tonsils by use of a forceps and scissors with a wire loop called a 'snare' was formerly the most common method practiced by otolaryngologists, but has been largely replaced in favor of other techniques. The procedure requires the patient to undergo general anesthesia; the tonsils are completely removed and the remaining tissue surface is cauterized. The patient will leave with minimal post-operative bleeding.
- Electrocautery: Electrocautery uses electrical energy to separate the tonsillar tissue and assists in reducing blood loss through cauterization. Research has shown that the heat of electrocautery (400 °C) may result in thermal injury to surrounding tissue. This may result in more discomfort during the postoperative period.
- Radiofrequency ablation: Monopolar radiofrequency thermal ablation transfers radiofrequency energy to the tonsil tissue through probes inserted in the tonsil. The procedure can be performed in an office (outpatient) setting under light sedation or local anesthesia. After the treatment is performed, scarring occurs within the tonsil causing it to decrease in size over a period of several weeks. The treatment can be performed several times. The advantages of this technique are minimal discomfort, ease of operations, and immediate return to work or school. Tonsillar tissue remains after the procedure but is less prominent. This procedure is recommended for treating enlarged tonsils and not chronic or recurrent tonsillitis.
- Coblation tonsillectomy: This surgical procedure is performed using plasma to remove the tonsils. Coblation technology combines radiofrequency energy and saline to create a plasma field. The plasma field is able to dissociate molecular bonds of target tissue while remaining relatively cool (40-70 °C),[19] which results in minimal or no damage to surrounding healthy tissue. A Coblation tonsillectomy is carried out in an operating room setting, with the patient under general anesthesia. Tonsillectomies are generally performed for two main reasons: tonsillar hypertrophy (enlarged tonsils) and recurrent tonsillitis. It has been claimed that this technique results in less pain, faster healing, and less post operative care.[20] However, review of 21 studies gives conflicting results about levels of pain, and its comparative safety has yet to be confirmed.[21] This technique has been criticized for a higher than expected rate of bleeding presumably due to the low temperature which may be insufficient to seal the divided blood vessels but several papers offer conflicting (some positive, some negative) results. More recent studies of coblation tonsillectomy indicate reduced pain and ostalgia;[22] less intraoperative or postoperative complications;[23] lesser incidence of delayed hemorrhage, more significantly in pediatric populations,[24][25][26] less postoperative pain and early return to daily activities, fewer secondary infections of the tonsil bed and significantly lower rates of secondary hemorrhage.[27] Unlike the electrosurgery procedure, Coblation Tonsillectomy generates significantly lower temperatures on contacted tissue.[28] Long term studies seem to show that surgeons experienced with the technique have very few complications.
- Harmonic scalpel: This medical device uses ultrasonic energy to vibrate its blade at 55kHz. Invisible to the naked eye, the vibration transfers energy to the tissue, providing simultaneous cutting and coagulation. The temperature of the surrounding tissue reaches 80 °C. Proponents of this procedure assert that the end result is precise cutting with minimal thermal damage.
- Thermal Welding: A new technology which uses pure thermal energy to seal and divide the tissue. The absence of thermal spread means that the temperature of surrounding tissue is only 2-3 °C higher than normal body temperature. Clinical papers show patients with minimal post-operative pain (no requirement for narcotic pain-killers), zero edema (swelling) plus almost no incidence of bleeding. Hospitals in the US are advertising this procedure as "Painless Tonsillectomy". Also known as Tissue Welding.
- Carbon dioxide laser: When a laser is used to perform tonsillectomy, this is called laser-assisted serial tonsillectomy (LAST).[29] This is different from procedures where a laser is used to reduce or resurface the tonsils (e.g. laser cryptolysis). Providing the absence of certain contra-indications such as sensitive gag-reflex, LAST can be performed under local anesthetic as an outpatient procedure. A carbon dioxide laser is commonly used, and is swept over each tonsil 8–10 times. The smoke is aspirated out of the mouth to prevent smoke inhalation. Often, more than one procedure is required, each lasting about 20 minutes. The pain following LAST may be greater than other tonsillectomy methods. Due to the frequent requirement for multiple sessions, this treatment may work out more expensive than a single session tonsillectomy. A degree of patient compliance is required, making it unsuitable for young children and anxious persons, who risk harm if they move during the procedure.[29]
- Microdebrider: The microdebrider is a powered rotary shaving device with continuous suction often used during sinus surgery. It is made up of a cannula or tube, connected to a hand piece, which in turn is connected to a motor with foot control and a suction device. The endoscopic microdebrider is used in performing a partial tonsillectomy, by partially shaving the tonsils. This procedure entails eliminating the obstructive portion of the tonsil while preserving the tonsillar capsule. A natural biologic dressing is left in place over the pharyngeal muscles, preventing injury, inflammation, and infection. The procedure results in less post-operative pain, a more rapid recovery, and perhaps fewer delayed complications. However, the partial tonsillectomy is suggested for enlarged tonsils – not those that incur repeated infections.
Post-operative care
A sore throat will persist approximately two weeks following surgery while pain following the procedure is significant and may necessitate a hospital stay.[30] Recovery can take from 7 to 10 days and proper hydration is very important during this time, since dehydration can increase throat pain, leading to a vicious circle of poor fluid intake.[31][32]
At some point, most commonly 7–11 days after the surgery (but occasionally as long as two weeks (14 days) after), bleeding can occur when scabs begin sloughing off from the surgical sites. The overall risk of bleeding is approximately 1–2%. It is higher in adults, especially males over age 70 and three quarters of bleeding incidents occur on the same day as the surgery.[33] Approximately 3% of adult patients develop significant bleeding at this time which may sometimes require surgical intervention.
Post-operative pain relief is subject to change. Traditionally, pain relief has been provided by relatively mild narcotic analgesics such as Acetaminophen with codeine, for milder pain, and stronger narcotic analgesics for more severe pain. Recently (January 2011), the FDA reduced the recommended total 24-hour dose because of concern about liver toxicity from the Acetominophen component. An alternative is the use of non-steroidal anti-inflammatory agents, themselves giving rise to concerns that their effect on platelets might increase the risk of post-operative bleeding.[34] In turn, this has renewed interest in techniques other than traditional 'extra-capsular excision' in the hope that post-operative pain might be reduced.[35]
Tonsillectomy appears to be more painful in adults than children, although there will be individual variations in response.[36]
Frequency
More than 530,000 procedures are performed annually in children younger than 15 years in the United States.[4] The current tonsillectomy "rate" is 0.53 per thousand children and 1.46 per thousand children for combined tonsillectomy and adenoidectomy.[37]
History
Tonsillectomy has been practiced for 2,000 years, with varying popularity over the centuries.[38] The procedure is claimed in some books as "Hindu medicine" about 1000 BC (non-evidence based literature). Others refer to it as cleaning of tonsil using the nail of the index finger. Roughly a millennium later the Roman aristocrat Aulus Cornelius Celsus (25 BC – 50 AD) described a procedure whereby using the finger (or a blunt hook if necessary), the tonsil was separated from the neighboring tissue before being cut out.[38] Galen (121–200 AD) was the first to advocate the use of the surgical instrument known as the snare, a practice that was to become common until Aetius (490 AD) recommended partial removal of the tonsil, writing "Those who extirpate the entire tonsil remove, at the same time, structures that are perfectly healthy, and, in this way, give rise to serious Hæmorrhage".[38] In the 7th century Paulus Aegineta (625–690) described a detailed procedure for tonsillectomy, including dealing with the inevitable post-operative bleeding. 1,200 years pass before the procedure is described again with such precision and detail.[38]
The Middle Ages saw tonsillectomy fall into disfavor; Ambroise Pare (1509) wrote it to be "a bad operation" and suggested a procedure that involved gradual strangulation with a ligature. This method was not popular with the patients due to the immense pain it caused and the infection that usually followed. Scottish physician Peter Lowe in 1600 summarized the three methods in use at the time, including the snare, the ligature, and the excision.[38] At the time, the function of the tonsils was thought to be absorption of secretions from the nose; it was assumed that removal of large amounts of tonsillar tissue would interfere with the ability to remove these secretions, causing them to accumulate in the larynx, resulting in hoarseness. For this reason, physicians like Dionis (1672) and Lorenz Heister censured the procedure.

In 1828, physician Philip Syng Physick modified an existing instrument originally designed by Benjamin Bell for removing the uvula; the instrument, known as the tonsil guillotine (and later as a tonsillotome), became the standard instrument for tonsil removal for over 80 years.[38] By 1897, it became more common to perform complete rather than partial removal of the tonsil after American physician Ballenger noted that partial removal failed to completely alleviate symptoms in a majority of cases. His results using a technique involving removal of the tonsil with a scalpel and forceps were much better than partial removal; tonsillectomy using the guillotine eventually fell out of favor in America.[38]
Image gallery
 Throat with tonsilloliths.
Throat with tonsilloliths.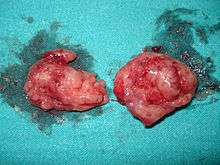 Two removed tonsils.
Two removed tonsils. Throat 1 day after a tonsillectomy.
Throat 1 day after a tonsillectomy. Throat some days after a tonsillectomy.
Throat some days after a tonsillectomy.
See also
Footnotes
- ↑ Paradise JL (1983). "Tonsillectomy and Adenoidectomy" (PDF). Pediatric otolaryngology: 122–6.
- ↑ American Academy of Otolaryngology—Head and Neck Surgery. 2012 Clinical Indicators Compendium. Clinical Indicators: Tonsillectomy, Adenoidectomy, Adenotonillectomy.
- ↑ Svoboda, Elizabeth (31 August 2009). "In Tonsils, a Problem the Size of a Pea". The New York Times. Retrieved 8 January 2011.
- 1 2 Baugh RF, Archer SM, Mitchell RB, Rosenfeld RM, Amin R, Burns JJ, Darrow DH, Giordano T, Litman RS, Li KK, Mannix ME, Schwartz RH, Setzen G, Wald ER, Wall E, Sandberg G, Patel MM (January 2011). "Clinical practice guideline: tonsillectomy in children". Otolaryngology-Head and Neck Surgery. 144 (1 Suppl): S1–30. doi:10.1177/0194599810389949. PMID 21493257.
- ↑ Randel, A (1 September 2011). "AAO-HNS Guidelines for Tonsillectomy in Children and Adolescents.". American family physician. 84 (5): 566–73. PMID 21888309.
- ↑ Blakley, BW, Magit A (2009). "Response to: The role of tonsillectomy in reducing recurrent pharyngitis: A systematic review, from Jeremy Hornibrook". Otolaryngology-Head and Neck Surgery. 141 (1): 155–156. doi:10.1016/j.otohns.2009.04.017.
- ↑ Blakley, BW; Magit, AE (March 2009). "The role of tonsillectomy in reducing recurrent pharyngitis: a systematic review". Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 140 (3): 291–7. doi:10.1016/j.otohns.2008.12.013. PMID 19248931.
- 1 2 Burton, Martin J.; Glasziou, Paul P.; Chong, Lee Yee; Venekamp, Roderick P. (2014-01-01). "Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis". The Cochrane Database of Systematic Reviews. 11: CD001802. doi:10.1002/14651858.CD001802.pub3. ISSN 1469-493X. PMID 25407135.
- ↑ Marshall T (1998). "A review of tonsillectomy for recurrent throat infection." (PDF). British Journal of General Practice. 48 (431): 1331–1335. PMC 1410132
 . PMID 9747553.
. PMID 9747553. - ↑ Paradise JL, et al. (2002). "Tonsillectomy and adenotonsillectomy for recurrent throat infection in moderately affected children.". Pediatrics. 110 (1): 7–15. doi:10.1542/peds.110.1.7. PMID 12093941.
- ↑ Marshall T (2002). "Effectiveness of tonsillectomy? A reply to Howel et al". Family Practice. 19 (1): 707–708. doi:10.1093/fampra/19.6.707-a. PMID 12429681.
- ↑ Marshall T, et al. (2001). "How many tonsillectomies are evidence-based?". Journal of Clinical Excellence. 3 (5): 23–25.
- 1 2 3 Steward, DL; Grisel, J; Meinzen-Derr, J (10 August 2011). Steward, David L, ed. "Steroids for improving recovery following tonsillectomy in children". Cochrane database of systematic reviews (Online) (8): CD003997. doi:10.1002/14651858.CD003997.pub2. PMID 21833946.
- ↑ Wijga, AH; Scholtens, S; Wieringa, MH; Kerkhof, M; Gerritsen, J; Brunekreef, B; Smit, HA (Apr 2009). "Adenotonsillectomy and the development of overweight.". Pediatrics. 123 (4): 1095–101. doi:10.1542/peds.2008-1502. PMID 19336367.
- ↑ Wei, JL (Jun 2011). "Weight gain after tonsillectomy: myth or reality? Interpreting research responsibly.". Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 144 (6): 855–7. doi:10.1177/0194599811406674. PMID 21515804.
- ↑ Lee KL, p. 544.
- ↑ Walton J, Ebner Y, Stewart MG, April MM (2012). "Systematic Review of Randomized Controlled Trials Comparing Intracapsular Tonsillectomy With Total Tonsillectomy in a Pediatric Population". Arch Otolaryngol Head Neck Surg. 138 (3): 243–49. doi:10.1001/archoto.2012.16. PMID 22431869.
- ↑ Koempel JA, Solares CA, Koltai PJ (December 2006). "The evolution of tonsil surgery and rethinking the surgical approach to obstructive sleep-disordered breathing in children". J Laryngol Otol. 120 (12): 993–1000. doi:10.1017/S0022215106002544. PMID 16923328.
- ↑ "COBLATION Plasma Technology - ENT". Smith & Nephew US Professional. Retrieved 15 July 2016.
- ↑ Friedman M, LoSavio P, Ibrahim H, Ramakrishnan V (2003). "Radiofrequency tonsil reduction: safety, morbidity, and efficacy". Laryngoscope. 113 (5): 882–7. doi:10.1097/00005537-200305000-00020. PMID 12792327.
- ↑ Windfuhr JP. (2007). "[Coblation tonsillectomy: a review of the literature.]". HNO. 55 (5): 337–48. doi:10.1007/s00106-006-1523-3. PMID 17431570.
- ↑ Sun-Moon, Hong (June 14, 2013). "Coblation vs. Electrocautery Tonsillectomy: A Prospective Randomized Study Comparing Clinical Outcomes in Adolescents and Adults". Clinical and Experimental Otorhinolaryngology. 6 (2): 90. doi:10.3342/ceo.2013.6.2.90.
- ↑ Omrani, M (January 2012). "Coblation versus traditional tonsillectomy: A double blind randomized controlled trial". Journal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences. 17 (1): 45–50. PMC 3523437. PMID 23248656.
- ↑ Walner, DL (October 1, 2012). "Coblation tonsillectomy in children: incidence of bleeding.". Laryngoscope. 122 (10): 2330–6. doi:10.1002/lary.23526. PMID 22833366.
- ↑ Kahn, I (February 4, 2012). "Coblation tonsillectomy: is it inherently bloody?". Eur Arch Otorhinolaryngology. 269 (2): 579–83. doi:10.1007/s00405-011-1609-8. PMID 21547390.
- ↑ Mosges, R (June 5, 2011). "Hemorrhage rate after coblation tonsillectomy: a meta-analysis of published trials.". Eur Arch Otorhinolaryngology. 286 (6): 807–16. doi:10.1007/s00405-011-1535-9. PMC 3087106. PMID 21373898.
- ↑ Beloso, A (November 2003). "Coblation tonsillectomy versus dissection tonsillectomy: postoperative hemorrhage". Laryngoscope. 113 (11).
- ↑ "COBLATION Tonsillectomy - My Tonsils". My Tonsils.com. Retrieved 11 July 2016.
- 1 2 "Interventional procedure overview of laser assisted serial tonsillectomy" (PDF). National institute of clinical excellence. Retrieved 30 November 2013.
- ↑ Graham, John M.; Glenis K. Scadding; Peter D. Bull (2008). Pediatric ENT. Springer. p. 136. ISBN 3-540-69930-9.
- ↑ Timby, Barbara Kuhn; Nancy Ellen Smith (2006). Introductory medical-surgical nursing. Lippincott Williams & Wilkins. p. 357. ISBN 0-7817-8032-2.
- ↑ Pemberton, Cecilia M. (1988). Mayo Clinic diet manual. B.C. Decker. ISBN 1-55664-032-3.
- ↑ Windfuhr JP, Chen YS, Remmert S (2005). "Hemorrhage following tonsillectomy and adenoidectomy in 15,218 patients". Otolaryngology-Head and Neck Surgery. 132 (2): 281–86. doi:10.1016/j.otohns.2004.09.007. PMID 15692542.
- ↑ Møiniche S, Rømsing J, Dahl JB, Tramèr MR (January 2003). "Nonsteroidal antiinflammatory drugs and the risk of operative site bleeding after tonsillectomy: a quantitative systematic review". Anesth Analg. 96 (1): 68–77. doi:10.1213/00000539-200301000-00015. PMID 12505926.
- ↑ Chimona T, Proimos E, Mamoulakis C, Tzanakakis M, Skoulakis CE, Papadakis CE (September 2008). "comparison of cold knife tonsillectomy, radiofrequency excision and thermal welding tonsillectomy in children". Int J Pediatr Otorhinolaryngol. 72 (9): 1431–6. doi:10.1016/j.ijporl.2008.06.006. PMID 18620759.
- ↑ Graumüller S, Laudien B (November 2003). "Postoperative pain after tonsillectomy—comparison of children and adults". Advances in Pediatric ORL. Proceedings of the 8th International Congress of Pediatric Otorhinolaryngology. 1254: 469–72. doi:10.1016/S0531-5131(03)01073-2.
- ↑ Bhattacharyya N, Lin HW (November 2010). "Changes and consistencies in the epidemiology of pediatric adenotonsillar surgery". Otolaryngology-Head and Neck Surgery. 43 (5): 680–4. doi:10.1016/j.otohns.2010.06.918. PMID 20974339.
- 1 2 3 4 5 6 7 McNeill RA., RA (1 June 1960). "A History of Tonsillectomy: Two Millenia of Trauma, Hæmorrhage and Controversy". Ulser Medical Journal. 29 (1): 59–63. PMC 2384338. PMID 20476427.
References
- Kramer SP, Pasha R (2005). Otolaryngology: Head and Neck Surgery--A Clinical & Reference Guide, Second Edition. Plural Publishing. ISBN 1-59756-023-5.
- Lee KL. (2008). Essential Otolaryngology: Head and Neck Surgery, Ninth Edition. McGraw-Hill Professional. ISBN 0-07-148270-9.
- Montgomery WR. (1996). Surgery of the Upper Respiratory System. Baltimore: Williams & Wilkins. ISBN 0-683-06121-6.
- Nsow JB.; Wackym PA. (2009). Ballenger's Otorhinolaryngology Head and Neck Surgery, 17th edition (Otorhinolaryngology: Head and Neck Surgery (Ballenger)). pmph usa. ISBN 1-55009-337-1.
- "Clinical UM Guideline CG-SURG-30: Tonsillectomy for Children".
External links
| Wikimedia Commons has media related to Tonsillectomy. |
- Tonsillectomy Procedures
- ENT Matters: Tonsillectomy
- drtbalu otolaryngology on line
- History of tonsillectomy
- Tonsillectomy new vistas
- Laser Tonsillectomy Procedure