Subclavian steal syndrome
| Subclavian steal syndrome | |
|---|---|
| Classification and external resources | |
| Specialty | neurology |
| ICD-10 | G45.8 |
| ICD-9-CM | 435.2 |
| DiseasesDB | 31525 |
| eMedicine | article/418203 article/462036 |
| MeSH | D013349 |
In medicine, subclavian steal syndrome (SSS), also called subclavian steal phenomenon or subclavian steal steno-occlusive disease, is a constellation of signs and symptoms that arise from retrograde (reversed) blood flow in the vertebral artery or the internal thoracic artery, due to a proximal stenosis (narrowing) and/or occlusion of the subclavian artery. The arm may be supplied by blood flowing in a retrograde direction down the vertebral artery at the expense of the vertebrobasilar circulation. This is called the subclavian steal. It is more severe than typical vertebrobasilar insufficiency.
Pathophysiology
Classically, SSS is a consequence of a redundancy in the circulation of the brain[1][2] and the flow of blood.
SSS results when the short low resistance path (along the subclavian artery) becomes a high resistance path (due to narrowing) and blood flows around the narrowing via the arteries that supply the brain (left and right vertebral artery, left and right internal carotid artery). The blood flow from the brain to the upper limb in SSS is considered to be stolen as it is blood flow the brain must do without. This is because of collateral vessels.
As in vertebral-subclavian steal, coronary-subclavian steal may occur in patients who have received a coronary artery bypass graft using the internal thoracic artery (ITA), also known as internal mammary artery.[3] As a result of this procedure, the distal end of the ITA is diverted to one of the coronary arteries (typically the LAD), facilitating blood supply to the heart. In the setting of increased resistance in the proximal subclavian artery, blood may flow backward away from the heart along the ITA, causing myocardial ischemia due to coronary steal. Vertebral-subclavian and coronary-subclavian steal can occur concurrently in patients with an ITA CABG.[4]
Hemodynamics
Blood, like electric current, flows along the path of least resistance. Resistance is affected by the length and width of a vessel (i.e. a long, narrow vessel has the greatest resistance and a short, wide one the least), but crucially in the human body width is generally more limiting than length because of Poiseuille's Law. Thus, if blood is presented with two paths, a short one that is narrow (with a high overall resistance) and a long one that is wide (with a low overall resistance), it will take the long and wide path (the one with the lower resistance).
Vascular anatomy
The blood vessels supplying the brain arise from the vertebral arteries and internal carotid arteries and are connected to one another by communicating vessels that form a circle (known as the Circle of Willis).
Path of the blood (normal versus SSS)
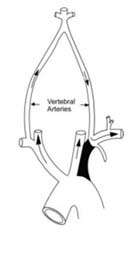
Normally, blood flows from the aorta into the subclavian artery, and then some of that blood leaves via the vertebral artery to supply the brain.
In SSS a reduced quantity of blood flows through the proximal subclavian artery. As a result, blood travels up one of the other blood vessels to the brain (the other vertebral or the carotids), reaches the basilar artery or goes around the cerebral arterial circle and descends via the (contralateral) vertebral artery to the subclavian (with the proximal blockage) and feeds blood to the distal subclavian artery (which supplies the upper limb and shoulder).
Etiology
Signs and symptoms
- Presyncope (sensation that one is about to faint)
- Syncope (fainting)
- Neurologic deficits
- Blood pressure differential between the arms
- severe memory problems
- hands showing circulation problems (hands can have blotchy patches of red and white) (associated with other stigmata of vascular disease (e.g. vascular insufficiency ulcers of the foot).
Differential diagnosis
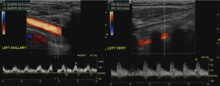
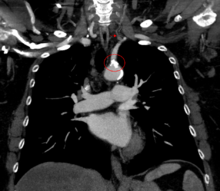
Diagnostic tests

Treatment
See also
References
- ↑ Klingelhöfer J, Conrad B, Benecke R, Frank B (1988). "Transcranial Doppler ultrasonography of carotid-basilar collateral circulation in subclavian steal.". Stroke. 19 (8): 1036–42. doi:10.1161/01.STR.19.8.1036. PMID 3041649.
- ↑ Lord R, Adar R, Stein R (1969). "Contribution of the circle of Willis to the subclavian steal syndrome". Circulation. 40 (6): 871–8. doi:10.1161/01.CIR.40.6.871. PMID 5377222.
- ↑ Takach T, Reul G, Cooley D, Duncan J, Livesay J, Ott D, Gregoric I (2006). "Myocardial thievery: the coronary-subclavian steal syndrome". Ann Thorac Surg. 81 (1): 386–92. doi:10.1016/j.athoracsur.2005.05.071. PMID 16368420.
- ↑ Lee S, Jeong M, Rhew J, Ahn Y, Na K, Song H, Bom H, Cho J, Ahn B, Park J, Kim S, Kang J (2003). "Simultaneous coronary - subclavian and vertebral - subclavian steal syndrome". Circ J. 67 (5): 464–6. doi:10.1253/circj.67.464. PMID 12736489.
External links
- Subclavian Steal Syndrome - emedicine.com